By Archit Vora, Zheng Cheng Zhu
Key reference:
Chua MJ, Lersch F, Chua AWY, Kumar CM, Eke T. Sub-Tenon’s anaesthesia for modern eye surgery-clinicians’ perspective, 30 years after re-introduction. Eye (Lond). 2021;35(5):1295-1304. doi:10.1038/s41433-021-01412-5
Demonstration of sub-Tenon block can be found on ABCs of Anaesthesia Youtube channel:
https://www.youtube.com/watch?v=k_bxA9GiGNs
Quick Summary
-
Contemporary ophthalmic surgeries are increasingly being performed under regional and local anaesthesia with non-inferior analgesia, akinesia, safety profile and improved efficiency in list turnover.
-
The sub-Tenon block (STB) presents an effective modality to achieve ocular analgesia and akinesia with superior safety profile compared to needle-based peribulbar and retrobulbar techniques.
-
STB is associated with common but self-limiting complications including chemosis and subconjunctival haemorrhage.
-
Nevertheless, retrobulbar haemorrhage (RBH), a sight-threatening ocular emergency resulting from rapid increases in intraocular pressure (IOP) from accumulated retrobulbar blood, remains a rare complication of STB.
-
Prompt recognition of RBH is essential to expedite definitive lateral canthotomy decompression and minimise long-term sight impairment.
Preamble
You are a junior anaesthetic trainee on your first busy ophthalmology list. Your next patient is Mrs. CS, a 70 year old lady who has arrived for her elective left eye cataract surgery. She had her right eye cataract completed 2 months ago without any issues.
Her history is significant for ischaemic heart disease and atrial fibrillation, for which she is on aspirin 100mg daily and apixaban 2.5mg BD. Her preoperative visual acuity (VA) was 6/6 for right eye and hand movements-only for left eye. Both eyes had deep anterior chamber depths. Baseline IOP was 26mmHg for the right eye. After an unremarkable preoperative assessment, the patient was consented for a sub-Tenon block (STB).
What is a sub-Tenon Block (STB)?
STB is a regional eye block technique developed in 1884 and popularised in the 1990s. In contrast to needle-based peribulbar and retrobulbar blocks, STB utilises blunt-end cannula to deliver local anaesthetics into the episcleral potential space, targeting both sensory ocular nerves and all 6 extraocular muscle sheaths to produce anaesthesia and akinesia.
Tenon’s capsule is the fascial sheath that surrounds the globe. Anteriorly, it merges with the conjunctiva at the limbus, and posteriorly fusing with the meninges and sclera of the optic nerve. Between the Tenon’s capsule and the sclera contains the episcleral potential space, which is transverse by:
|
Vessels |
Short ciliary arteries
Vortex veins x4
|
|
Nerves |
Posterior ciliary nerves
|
|
Muscle |
Extraocular muscle sheath x6
|
To access the sub-Tenon space, the infero-nasal quadrant is favoured as it is least likely to be traversed by the vortex veins or other neurovascular and muscular structures.
Once administered, the local anaesthetic hydro-dissects the episcleral space and creates a circumferential collection bathing the ciliary nerves. With larger volumes (>3mls), local anaesthetic spreads along the extraocular muscle sheath, as well as anteriorly to the facial plane of the lid to provide akinesia of the globe and eyelid muscles.

Steps to completing a STB
-
Patient consent
-
Position patient supine position
-
WHO block timeout
-
Standard ANZCA monitoring
-
IV access +/- anxiolysis/sedation if necessary, with IV midazolam/low dose propofol/ fentanyl
-
Hat/mask/sterile glove
-
2-3 drops of topical anaesthetics of choice to target eye (e.g. 0.4% oxybuprocaine)
-
Skin prep with iodine-based antiseptic (e.g. betadine 1% solution), followed by sterile drape
-
Apply eye speculum
-
Ask patient to look superotemporally with the target eye to expose the inferonasal quadrant
-
Create a small tent of conjunctiva 5-7mm from the limbus using a conjunctival forceps (e.g. Moorfield’s), and make a small incision using Wescott spring scissors
-
Non-snip techniques are also available using pencil point cannula or other plastic probes
-
-
Insert the blunt-end sub-Tenon cannula through the incision and up to the globe equator in depth, always hugging the sclera during the insertion
-
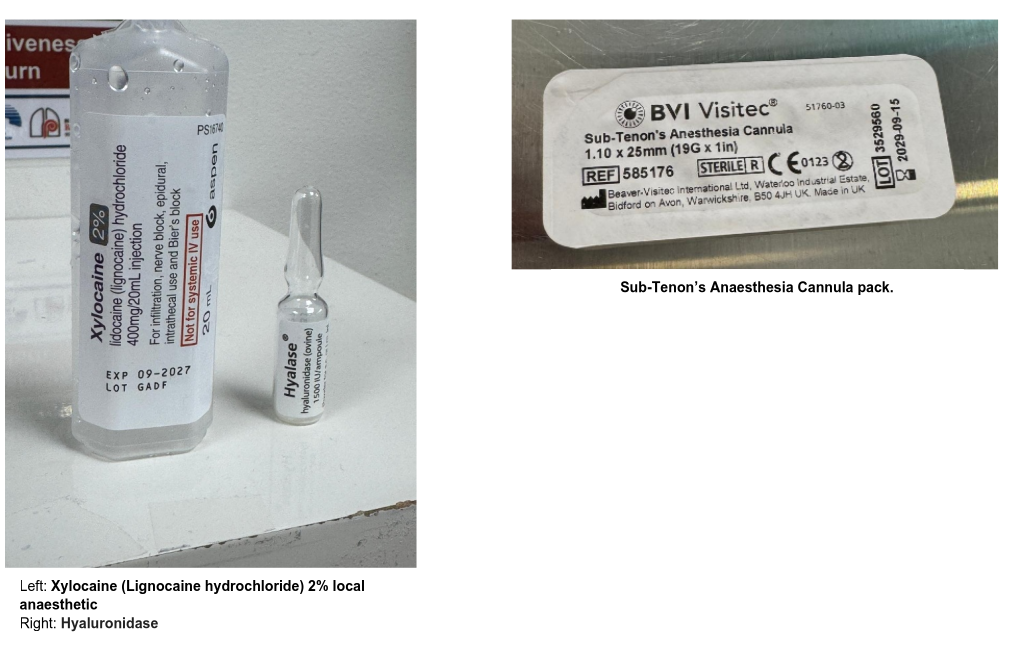
Slowly inject 3-5ml of local anaesthetic solution of choice into the sub-Tenon space (e.g. 2% lidocaine with 30 units/ml hyaluronidase), avoiding injecting if high resistance or discomfort encountered
-
Hyaluronidase hydrolyses part of the extracellular matrix, improves local anaesthetic dispersion and penetration, reduces volume of LA required, and reduces time for onset of akinesia
-
-
Perform a post-block assessment, noting any immediate complications (e.g. chemosis, subconjunctival haemorrhage), pain, discomfort, periorbital swelling, proptosis etc.)
Sub-Tenon Block set up and equipment

Who is suitable for STB?
STB and other needle-based regional techniques are allowing patients to undergo low-risk ophthalmic procedures who would otherwise be at significant high risk for general anaesthetics. While STB is considered safe and effective for vast majority of patients, certain patient populations have relative and absolute contraindications to a STB:
|
Patient factors |
Patient non-consent
Inability to follow instructions
Inability to remain still while lying flat
Anticoagulant / antiplatelet therapy
|
|
Eye disease factors |
Active eye infection
Conjunctival / Tenon capsule scarring
Scleral thinning / staphyloma
Eye trauma
|
|
Surgical factors |
Akinesia requirements
|
Complications of STB
STB is a favoured eye block technique due to its superior safety profile. Two prospective studies in Australia and New Zealand with combined 8688 STBs observed no sight-threatening complications related to STBs. While STB is associated with higher rates of benign and transient complications such as chemosis and subconjunctival haemorrhage, sight and life-threatening complications are exceedingly rare and are 2.5 times less common than needle blocks. A Cochrane review of 605 patients undergoing cataract surgery found no evidence STB had a higher rate of intraoperative complications compared to non-invasive topical anaesthesia, albeit with limited statistical power.
|
Minor complications |
Major / sight-threatening complications |
|
Conjunctival haemorrhage
Chemosis
|
Sight threatening
Life threatening
|
…………………………..
Returning to Ms CS:
You successfully complete the STB for Mrs. CS in the holding bay. You note the patient’s bleeding risk whilst on both anticoagulant and antiplatelet therapy, but are reassured by your consultant of the low risk of sight threatening haemorrhage.
As you are waiting for the surgeons to prepare, Mrs CS reports increasing discomfort of the operative eye. You note that the eye has become tense with onset of periorbital swelling and resistance to retropulsion. Examination revealed proptosis of the right eye, with increased IOP up to 45mmHg. Your consultant immediately suspects a retrobulbar haemorrhage and reports to the ophthalmologist.
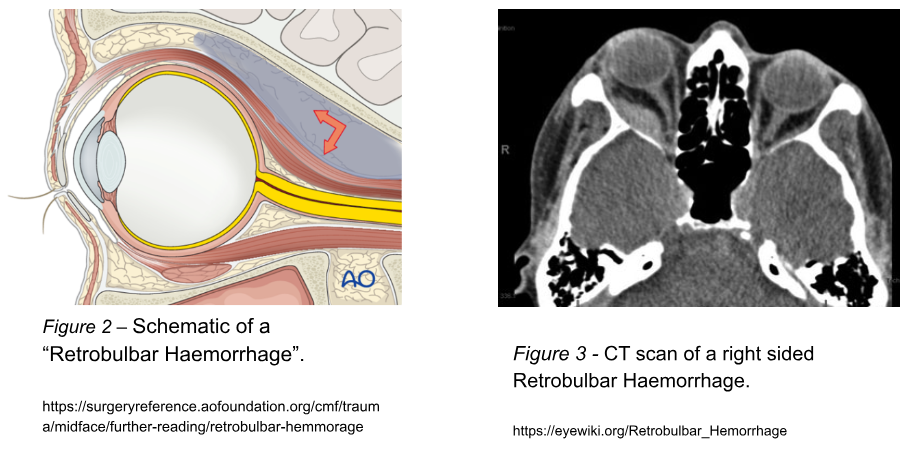
What is retrobulbar haemorrhage?
Retrobulbar haemorrhage (RBH) is a sight-threatening ophthalmic emergency, characterised by raised intraocular pressure (IOP) secondary to accumulating blood within the tight intraconal space, causing extrinsic compression of neurovascular structures, impairing orbital venous drainage and arterial supply, ultimately resulting in retinal ischaemia and optic nerve injury. RBH can be spontaneous, or through iatrogenic trauma such as with regional anaesthesia, which has a prevalence of 0.04% to 0.43%.
RBH is an extremely rare complication of STB, with isolated cases described in a small number of case reports and retrospective studies. The pathophysiology is attributed to iatrogenic injury to the vortex veins that traverses through the sub-Tenon space, causing slow ooze and gradual intraocular pressure rise. The use of metal cannulas, transient intraocular pressure rise from cough/Valsalva reflex, posterior vessel crowding from increased axial length, and use of antithrombotic therapy were respectively implicated as possible contributing factors. Due to the lack of case numbers, there is insufficient statistical power to-date to validate these risk factors.
Minimising RBH risk during STB
Using standard inferonasal approach
The inferonasal quadrant avoids the majority of neurovascular and muscular structures. Specifically, the vortex vein in the temporal region commonly loops around into the inner surface of the Tenon’s capsule, posterior to the insertion of the inferior rectus muscle. Thus, the inferonasal approach is usually preferred over inferotemporal to reduce the risk of vortex vein injury and RBH.
Using shorter, non-metal, blunt cannula
The vortex veins and ciliary vessels are concentrated in the posterior quadrant. As such, it is advisable to avoid cannula over-advancement beyond the globe equator and endangering posterior vascular structures. Anaesthetists should pay extra attention to the orbit’s axial length during their pre-operative assessment, which informs the required needle depth, as well as the risks of scleral thinning and irregularities. The use of shorter, flexible cannulas in favour of rigid metal cannulas has been suggested to avoid inadvertent vessel injury.
Using smaller local anaesthetic volume
Further risk minimisation through reducing volume (and speed of injection) of local anaesthetics to prevent shearing of sclerotic vessels and rise of intraocular pressure must be balanced with patient discomfort and suboptimal akinesia conditions associated with incomplete block.
Avoidance of “orbital massage”
Orbital massage is a technique used to disperse local anaesthetic throughout the sub-Tenon space by firm rocking pressure applied against the orbit. This has been shown to increase intraocular pressure abruptly to 400mmHg, significantly increasing shear stress on posterior vessels.
Management of RBH
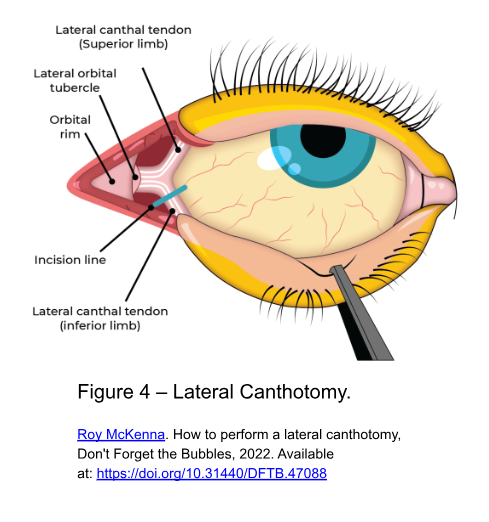
Management of RBH requires early recognition of intraocular pressure, which may present as eye pain, proptosis, periorbital swelling, visual disturbance, impaired eye movements, or increased IOP. Immediate surgical decompression via lateral canthotomy/cantholysis, with adjunct medical management to reduce IOP is the first line of management, and is associated with only 0.14% rate of blindness if instituted promptly. Medical management commonly involves administration of acetazolamide, corticosteroids, and topical timolol to decrease aqueous humor production in the eye to further reduce IOP.
Returning to Ms CS
The ophthalmologist immediately sets up and performs a lateral canthotomy and cantholysis in theatre, with you administering procedural sedation. A small pocket of blood is evacuated.
Within minutes, Ms. CS’s symptoms improved, and proptosis is visibly reduced. Reassessment of the IOP showed a pressure of 15 mmHg.
You arrange for Ms. CS to be transferred to a tertiary eye centre for overnight observations. You instruct her to withhold her apixaban and aspirin for today. You commence her on acetazolamide (500 mg IV) and topical timolol to control her IOP. Immediate post-procedure monitoring noted no further signs of rebleeding or worsening of symptoms.
Ms. CS is discharged the next day. She returns 1 week later to complete her cataract surgery under general anaesthesia without complication, and fully recovers her VA.
Conclusion
STB continues to be a popular, safe and effective regional technique for ophthalmic surgery. While major complications are extremely rare, anaesthetists must be vigilant of signs and symptoms and follow techniques that minimise their risk. In the case of suspected RBH, prompt action must be taken to prevent permanent vision loss through surgical and medical management.
References
Chua MJ, Lersch F, Chua AWY, Kumar CM, Eke T. Sub-Tenon’s anaesthesia for modern eye surgery-clinicians’ perspective, 30 years after re-introduction. Eye (Lond). 2021;35(5):1295-1304. doi:10.1038/s41433-021-01412-5
Clarke JP, Plummer J. Adverse Events Associated with Regional Ophthalmic Anaesthesia in an Australian Teaching Hospital. Anaesthesia and Intensive Care. 2011;39(1):61-64. doi:10.1177/0310057X1103900109
Ernest JT, Goldstick TK, Stein MA, Zheutlin JD. Ocular massage before cataract surgery. Trans Am Ophthalmol Soc. 1985; 83: 205–217.
Lerch D, Venter JA, James AM, Pelouskova M, Collins BM, Schallhorn SC. Outcomes and Adverse Events of Sub-Tenon’s Anesthesia with the Use of a Flexible Cannula in 35,850 Refractive Lens Exchange/Cataract Procedures. Clin Ophthalmol. 2020;14:307-315. Published 2020 Jan 31. doi:10.2147/OPTH.S234807
Subbiah S, McGimpsey S, Best RM. Retrobulbar hemorrhage after sub-Tenon’s anesthesia. J Cataract Refract Surg. 2007;33(9):1651-1652. doi:10.1016/j.jcrs.2007.04.042