Understanding perioperative hypothermia
By Dr Jessica Spurio
Key reference: Riley, C. and J. Andrzejowski (2018). “Inadvertent perioperative hypothermia.” BJA Education 18(8): 227-233.
Quick Summary
-
Hypothermia is defined as a core body temperature below 36°C.
-
Perioperative hypothermia is a common consequence of general and regional anaesthesia, occurring due to the effect of anaesthesia on thermoregulatory mechanisms.
-
It is associated with adverse outcomes such as increased risk of surgical site infections, increased bleeding, altered drug metabolism and adverse cardiac events.
-
Patients undergoing combined general and regional anaesthesia are at greatest risk.
-
Active warming using a forced air warming device is a practical technique for preventing or treating perioperative hypothermia and is recommended for all patients at risk.
Preamble
You are a resident starting your first week in anaesthesia. Your next patient is a 67 year old woman undergoing an elective laparoscopic cholecystectomy. Her past medical history includes hypertension and type 2 diabetes. She has a BMI of 35. Whilst reviewing her in the pre-operative bay, you look at her admission observations and notice her temperature is 35.8°C. How will this impact your anaesthetic management?

The Physiology of Thermoregulation
Core body temperature is tightly maintained within strict parameters (36.7°C – 37.1°C) to maintain optimal physiological conditions. Thermoregulation occurs via afferent input, central regulation and efferent responses.
Afferent Input: Heat and cold sensors located both peripherally (in skin and deep tissues) and centrally (in the brainstem, spinal cord and hypothalamus) relay thermal information to the brain via the lateral spinothalamic tract.
Central regulation: The hypothalamus is the primary thermoregulatory controller. It integrates input from sensors, and when a temperature outside of the targeted set point is detected, it triggers effector mechanisms to return the body to normothermia.
Effector mechanisms: These include both behavioural and autonomic responses.
-
Behavioural changes: changing clothing, altering ambient temperature or initiating voluntary movement.
-
Autonomic responses:
-
The main effectors are skin, skeletal muscle, sweat glands and brown adipose tissue,
-
Cooling mechanisms include vasodilation and sweating,
-
Warming mechanisms include vasoconstriction, non-shivering thermogenesis and shivering.
-
What are the effects of general and regional anaesthesia on thermoregulation?
Threshold temperature is the temperature at which an autonomic response is triggered.
Inter-threshold range is the range of core body temperatures between which no autonomic thermoregulatory effects are triggered.
Anaesthesia causes a reduced threshold temperature and therefore a widened inter-threshold range. This means that warming mechanisms are only triggered at much cooler body temperatures, in turn impairing the thermoregulatory response to hypothermia. .
In normal circumstances, the threshold temperature is 36.5°C for vasoconstriction and approximately 36°C for shivering. General anaesthesia reduces these thresholds by 2-3°C.
Furthermore, normal behavioural responses are completely eliminated during general anaesthesia, leaving patients reliant on already impaired autonomic responses.
Intraoperative hypothermia typically develops in a triphasic pattern
-
Rapid initial reduction in temperature as vasodilation occurs due to induction agents, leading to redistribution of body heat from core to peripheral tissues. Anaesthesia also reduces the activation threshold for thermoregulatory vasoconstriction.
-
Gradual, linear decline in temperature as heat loss via radiation, convection and evaporation exceeds metabolic heat production. Metabolic heat production is reduced by 15-40% during general anaesthesia.
-
Plateau phase as patients become hypothermic to the point of reaching the altered threshold for vasoconstriction. Maximal vasoconstriction occurs and the body begins to conserve heat.
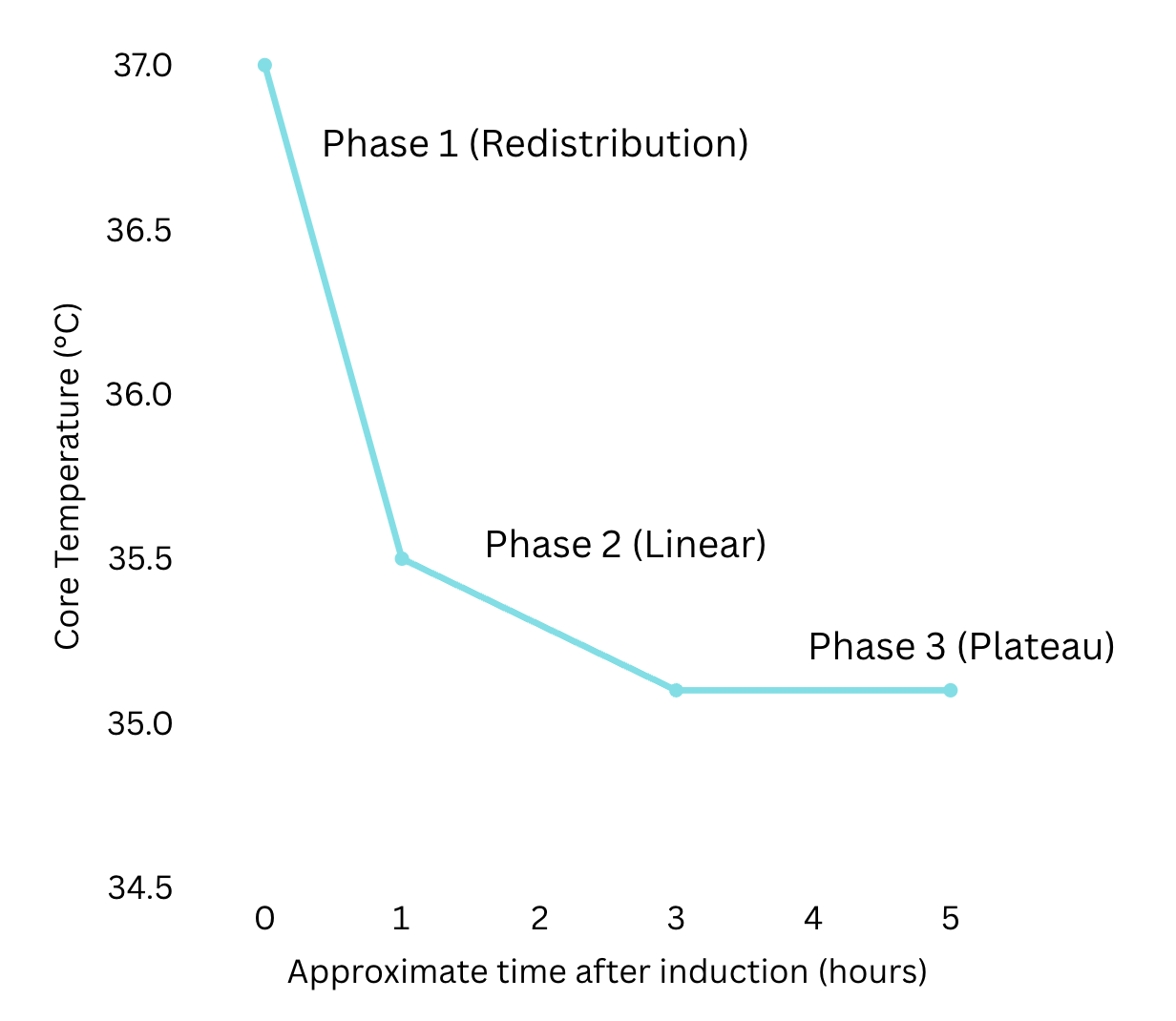
Figure 1: Characteristic triphasic pattern of intraoperative hypothermia
Measuring temperature: when and how?
Temperature should ideally be measured every 30 minutes in patients undergoing anaesthesia. Various devices may be used to measure temperature and these vary in their ability to provide an accurate estimate of core body temperature.
Most accurate
-
Pulmonary artery catheter (provides a highly accurate estimate of core temperature but is very invasive)
-
Lower oesophagus
-
Nasopharynx
-
Intravesical (In-dwelling catheter with temperature probe)
Less accurate
-
Tympanic
-
Axillary
-
Rectal
In modern day practice a nasopharyngeal temperature probe (thermistor) is used to continuously measure core temperature in patients under general anaesthesia.

Risk factors for perioperative hypothermia
Patient factors
-
ASA grade 2 – 5
-
Low BMI (higher surface area:volume ratio increases heat loss)
-
Elderly or paediatric patients
-
Pregnancy
-
Temperature < 36°C preoperatively
Surgical or anaesthesia factors
-
Major or emergency surgery
-
Duration of surgery > 30 minutes
-
Degree of body exposure
-
Theater ambient temperature < 21°C
-
Use of cold irrigation fluids
-
Combined general + regional anaesthesia
Risks and complications
|
Surgical site infections |
The risk of surgical site infections is increased via two mechanisms
|
|
Increased bleeding and transfusion requirements |
Due to hypothermia-induced impairment of platelet function and impairment of the coagulation cascade |
|
Altered drug metabolism |
Prolonged duration of action of neuromuscular blockers Increased tissue solubility of volatile anaesthetic agents -> delays onset and emergence from volatile anaesthetic Increased plasma concentration of propofol |
|
Cardiovascular complications |
Post-operative shivering causes a marked increase in oxygen demand whilst elevated catecholamine levels cause hypertension and increased myocardial workload |
|
Shivering |
Can increase postoperative pain Can make monitoring unreliable Can be distressing to patients |
Prevention and treatment
Before surgery
-
Identify high risk patients
-
Measure temperature preoperatively
-
Encourage patients to walk to theatre where possible
-
Ensure majority of patient’s body area is covered
-
Actively pre warm patients
During surgery/anaesthesia
-
Monitor temperature continuously
-
For anaesthesia expected to last >30 minutes, actively warm all high risk patients using forced air warming devices or heated blankets/mattresses
-
Ensure an ambient temperature of at least 21°C whilst the patient is exposed
-
Use warmed IV fluids and blood products (38-40°C)
After surgery
-
Monitor temperature in the PACU
-
Keep patients comfortably warm with blankets
-
Actively warm patients if their temperature is < 36°C

Conclusion
Let’s return to your next patient in the pre-operative bay. You identify that this patient has multiple risk factors for perioperative hypothermia including her pre-operative hypothermia and ASA grade of 2. You discuss the case with your consultant and propose a plan, which includes actively pre-warming the patient for at least 30 minutes before anaesthesia induction, ensuring warmed IV fluids are available to use during the case, continuing to warm the patient with a forced air warming device during the case and inserting an nasopharyngeal temperature probe to monitor her temperature. You communicate this plan with your anaesthetic nurse and your patient and proceed with the case. After wheeling her to PACU, you preemptively bring the forced air warming blanket together with her to ensure she remains warm until she fully emerges from her anaesthetic..
References
1. NICE guideline 65 Hypothermia: prevention and management in adults having surgery. 2008 [Available from: www.nice.org.uk/guidance/cg65
2. Bindu B, Bindra A, Rath G. Temperature management under general anesthesia: Compulsion or option. J Anaesthesiol Clin Pharmacol. 2017;33(3):306-16.
3. Doufas AG. Consequences of inadvertent perioperative hypothermia. Best Practice & Research Clinical Anaesthesiology. 2003;17(4):535-49.
4. Kirkbride DA, Buggy DJ. Thermoregulation and mild peri‐operative hypothermia. BJA CEPD Reviews. 2003;3(1):24-8.
5. Kurz A. Physiology of Thermoregulation. Best Practice & Research Clinical Anaesthesiology. 2008;22(4):627-44.
6. Riley C, Andrzejowski J. Inadvertent perioperative hypothermia. BJA Education. 2018;18(8):227-33.