By Ramis Hassan, Zheng Cheng Zhu
Key reference:
Athanassoglou V, Rogers A, Hofmeyr R. In-hospital management of the airway in trauma. BJA Educ. 2024;24(7):238-44. Available from: https://www.bjaed.org/article/S2058-5349(24)00031-3/fulltext
Preamble
You are the anaesthetic registrar on-call for a major trauma hospital. After your third morning coffee, your pager buzzes from ED resus for a trauma call.
On the resus bed is an e-scooter rider found unresponsive at the scene after colliding with a lamppost. Paramedics report a transient loss of consciousness and subsequent GCS of 8. Blood trickles from the patient’s nose, and a cervical collar sits snugly around their neck. The trauma team leader orders you to manage the airway.
On your primary survey
Critical haemorrhage
-
Nil external exsanguinating haemorrhage identified
A + Cspine
-
Partial obstruction with active oropharyngeal haemorrhage and soiling in unprotected airway,
-
Nil obvious red flag for aerodigestive / vascular neck injury
-
After suctioning, nil major distortion of maxillary-facial or oropharyngeal anatomy identified
-
Jaw movements not restricted,
-
Neck fixed in collar
B
-
Tachypnoea with oxygen saturation 92% on 6L hudson mask
-
Right sided consolidation on x-ray suggestive of aspiration, nil obvious pneumothorax
C
-
HR 105 bpm, BP 110/60mmHg
D
-
GCS 8 (E1 V2 M5)
-
Pupils right 3mm, left 5mm, reactive
“How do I manage this trauma airway?”

Airway management in trauma presents a unique challenge due to the critical and dynamic nature of these cases. This blog outlines a structured approach to in-hospital airway management for trauma patients. The focus is on preparation, early assessment, addressing anatomical and physiological complexities; by employing a variety of airway devices and techniques. Special considerations are needed where anatomical distortion and physiological instability add layers of complexity to airway management. While no approach can fully eliminate the unpredictability of trauma care, this exploration aims to aid and highlight tools to equip practitioners with greater confidence when facing these challenges.
Preparation
Managing a difficult trauma airway requires optimal environmental setup and team preparation, coordination and delegation. The team should have a clear, shared understanding of roles, priorities and checkpoints for escalation, with closed-loop communication and dynamic leadership to ensure the team can rapidly respond to deterioration.
Ideally, the trauma team should consist of Emergency physicians, Trauma Surgeons, Anaesthetists, the nursing team, and other teams as required. The trauma team should be assembled prior to the arrival of an injured patient; this allows for gathering of necessary personnel and equipment, role allocation and planning for management. The team leader (most often the Emergency physician) assigns roles, ensures the completion of the primary and secondary survey by coordinating between team members, and directs management priorities by maintaining a “hands-off” end-of-bed overview of the resuscitation.
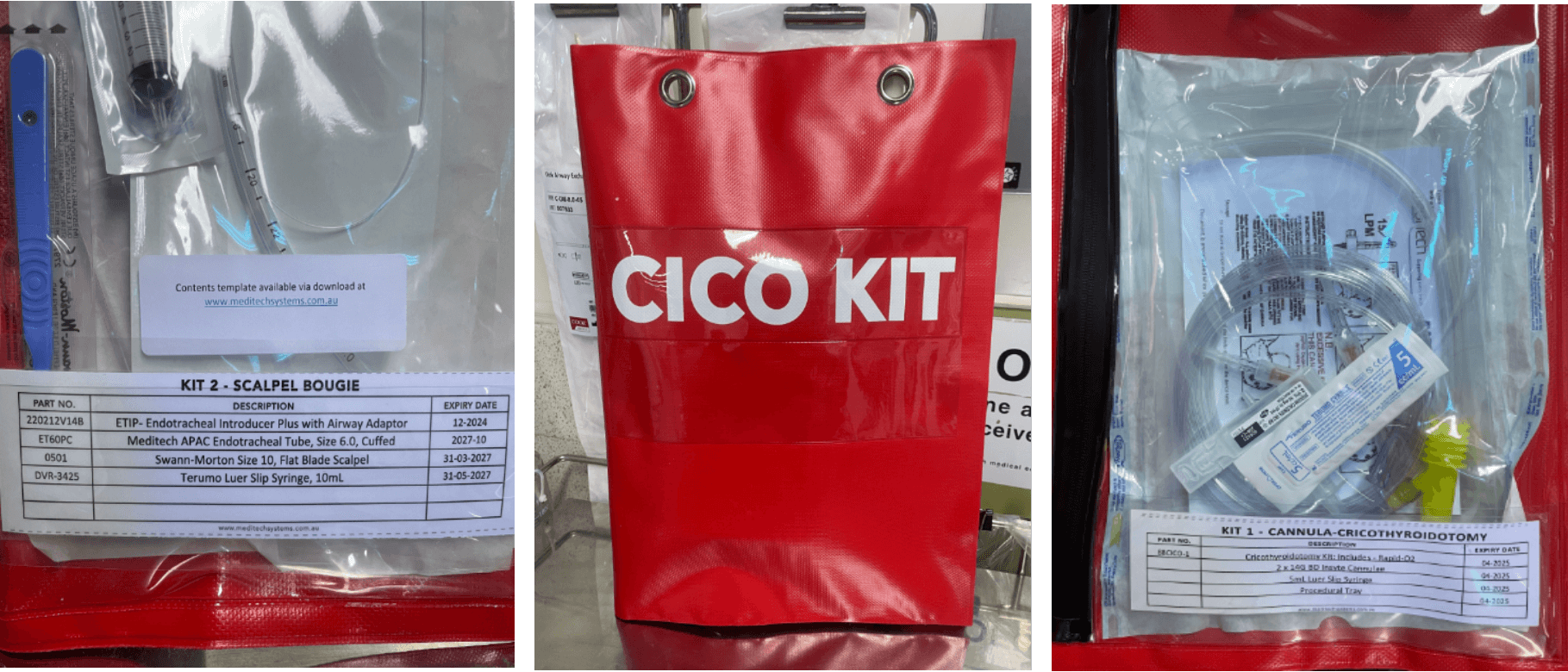
All airway management in trauma patients should be assumed to be difficult. Therefore, every effort should be made for equipment to be made readily available in the resuscitation area to deal with a soiled airway, difficult oxygenation and difficult laryngoscopy. An airway checklist should be used as a prompt prior to patient arrival to avoid critical omissions. It should also prompt the primary airway operator to verbalise their airway plans to establish a shared mental model and help quickly transition to contingency measures when difficulties are encountered. In most cases, additional personnel are required to provide manual inline stabilisation (MILS) or surgeons skilled in front-of-neck access.
Airway assessment
There may be limited time available for a comprehensive airway assessment before definitive management is required. Patients may be difficult to assess clinically.
Initial Evaluation:
-
Ensure a stable and patent airway while considering potential cervical spine injuries.
-
Early assessment includes identifying visible obstruction (blood, debris, swelling) and predicting anatomical challenges such as limited jaw mobility or airway distortion caused by maxillofacial and lower-airway trauma.
-
Large bore suction should be available to clear any debris.
Tools for Prediction:
-
Standardised frameworks like the modified LEMON scoring system (Look, Evaluate 3-3-2, Mallampati, Obstruction, Neck mobility) can be utilised to predict difficult laryngoscopy.
Note: Neck mobility cannot be assessed in patients in C-spine precautions.
Table 1. Modified LEMON assessment for predicting difficult laryngoscopy and tracheal intubation
|
Airway Assessment Component |
Criteria |
Points |
|
Look Externally |
Facial trauma, large incisors, beard or moustache, large tongue |
1 (for each) |
|
Evaluate the 3-3-2 |
Mouth opening < 3 finger breadths |
1 |
|
Hyomental distance < 3 finger breadths |
1 |
|
|
Thyrohyoid distance < 2 finger breadths |
1 |
|
|
Obstruction |
Presence of an obstructed airway |
1 |
|
Neck Mobility |
Presence of poor neck mobility |
1 |
|
Total (higher total predicts greater difficulty) |
/9 |
Dynamic Considerations
-
Oxygenation and ventilation are monitored continuously. Any deterioration in these parameters necessitates rapid adaptation of management strategies.
-
Predicting complications such as aspiration or airway collapse informs preparation for alternate techniques or emergency surgical airways.
Specialised Techniques
-
Flexible Naso-endoscopy (FNE), video laryngoscopy and fiberoptic techniques can be used to overcome limited visibility or anatomical distortion.
-
Airway ultrasound by trained operators can provide information such as identification of the depth and position of the cricothyroid membrane, trachea and pre-tracheal vessels as well as any relevant distorting features such as haematoma or other lesions.
Protection of the cervical spine
-
Cervical spine injuries (CSI) occur in 2-3% of patients after blunt force trauma.
-
There is a risk of exacerbation of CSI during the course of airway management.
-
The NEXUS and Canadian C-spine rules can be used to safely rule out C-spine injury without requiring radiographic imaging. (https://www.mdcalc.com/calc/696/canadian-c-spine-rule, https://pmc.ncbi.nlm.nih.gov/articles/PMC6494628/)
It is unlikely that trauma patients who require acute airway management will be able to have their cervical spine cleared without imaging.
-
Rigid collars are no longer recommended for in hospital cervical spine immobilisation as there is a lack of evidence of their efficacy and they carry an increased risk of pressure injuries and increase difficulty of airway management.
-
In hospital cervical spine immobilisation can be carried out using head blocks/rolls tape and a hard mattress.
Manual in-line stabilisation (MILS) is the recommended technique to stabilise the cervical spine during airway-management.
-
A dedicated assistant is required to align the patients head and neck in a neutral position and prevent inadvertent movements.
-
The assistant can crouch beside the intubator and cradle the patient’s mastoid processes and occiput.
-
MILS can also be done standing in-front of the intubator and beside the patient, with hands placed on the sides of the patient’s head and forearms resting on the patient’s chest.
-
Traction is not applied.
-
MILS improves the Cormack-Lehane grade in 56% of patients when their hard collar is removed and switched to a MILS technique.

Laryngoscopy:
-
Cervical spine immobilisation increases difficulty of laryngoscopy and intubation.
-
A Video Laryngoscope with a hyper-angulated blade is recommended as it does not require manual alignment of oral, pharyngeal and laryngeal axes
.
Tracheal intubation
Appropriate timing of intubation is key in trauma patients.
Indications for intubation
Patients can require intubation for a multitude of reasons; below are some common indications for intubation in trauma cases.
Airway
-
Unprotected airway
-
Airway obstruction (e.g., foreign bodies, bleeding into the mouth)
-
Airway trauma/burns
Breathing
-
Respiratory failure (e.g., respiratory arrest, poor oxygenation/ventilation)
Circulation
-
Severe haemodynamic instability (Intubation/sedation can help control the situation of an unpredictable unwell patient at risk of deterioration)
Disability
-
Altered GCS <8 (loss of protective airway reflexes)
-
Seizures
Environmental
-
Situational control for agitated or uncooperative patients
-
Facilitate further investigations or management (diagnostic/therapeutic procedures)
-
Stabilisation for transfer
Stabilising haemodynamics prior to intubation
-
Peri-intubation haemodynamic instability is common: encountered in up to 42% of critically ill patients undergoing emergency intubations.
-
It is essential to optimise resuscitation before induction and having fluids/blood, vasopressors and inotropes running or ready prior to administering induction agents.
-
Ensure adequate patient and equipment preparation, including at least 2x large bore IV access, standard monitoring (blood pressure, pulse oximetry, 3 lead ECG, end-tidal CO2), with consideration of invasive blood pressure monitoring and rapid infusion pumps, with blood products ready
Rapid Sequence Intubation (RSI)
Trauma patients undergoing emergency intubation are assumed to be unfasted and at risk of aspiration, warranting a RSI.
There is limited consensus over induction medications during a trauma RSI. However, case-specific selection of agents and doses should be carefully made based on haemodynamic state, pre-induction conscious state, comorbidities and suspected injuries.
-
IV anaesthetic agents include: Ketamine, midazolam, propofol and etomidate
-
Rapid onset Neuromuscular blocking drugs (NMBD) include: rocuronium: 1.2 mg/kg, suxamethonium: 1.5-2 mg/kg
-
Propofol is a potent sympatholytic that attenuates compensatory mechanisms and causes profound vasodilation, loss of preload/afterload, and increases the risk of haemodynamic collapse in a shocked patient.
-
Drastic dose reduction is often required in patients with altered GCS and haemodynamics to achieve safe anaesthesia.
In contrast to a “classical” RSI, trauma airways may require “modified” RSI techniques to improve patient safety
-
Patients with traumatic brain injury are susceptible to worsening intracranial hypertension with laryngoscopy-induced sympathetic reflex, and a neuro-protective induction should be employed.
-
There remains controversy over the efficacy of cricoid pressure and concerns of impeding laryngoscopic views. If injury is suspected to the airway or oesophagus then cricoid pressure should be avoided to prevent further damage to structures.
-
There is data to suggest that the risk of pulmonary aspiration is relatively lower compared to the risk of cardiovascular instability and severe hypoxaemia.The use of modified or delayed sequence RSI techniques, which allow for pressure limited mask ventilation prior to intubation, can be used to minimise peri-induction critical hypoxaemia and haemodynamic instability.
Pre-oxygenation
-
Delayed sequence intubation (DSI) involves a period of sedation to facilitate pre-oxygenation followed by induction dosage of hypnotic and NMBD agents. This approach is considered by weighing the risk of aspiration alongside the risk of failed intubation, agitation, cardiovascular instability and hypoxia.
-
If the airway is patent, then modalities for apnoeic oxygenation can be considered which include; high flow nasal oxygen (if not contraindicated), CPAP and pressure limited Bag-Mask-Valve (BMV) ventilation, to prolong safe apnoea time.
Theatre is a more appropriate setting if attempting awake intubation due to the patients’ injuries or pre-existing comorbidities. It requires a co-operative patient (often not the case in trauma patients), experienced anaesthetist and clinicians trained in front of neck access.
Optimisation of first-pass success
Achieving first-pass success is vital in trauma airway management.
-
Evidence shows first-pass intubation success is associated with a reduced likelihood of major adverse peri-intubation events
-
Each failed attempt increases the risk of hypoxia, aspiration, and haemodynamic instability.
-
If difficulty is encountered, oxygenating the patient should remain the priority.
Success is optimised by
-
Assigning the most airway experienced person for the first attempt.
-
Front loading technology; video laryngoscopy has been shown to increase first pass success and reduce rates of failed intubation.
-
Use of airway adjuncts (bougie/stylet) and BURP (if permitted)
-
Optimise positioning using 30-degree head up position. This is often difficult in trauma, acknowledging competing restrictions in place for spinal precautions.
-
The Difficult Airway Society (DAS) recommends a variety of strategies to enhance team performance including the use of team briefings, verbalising the mitigating strategies if initial management fails, minimising distractions and training team members in human factors such as graded assertiveness.
Managing the soiled airway
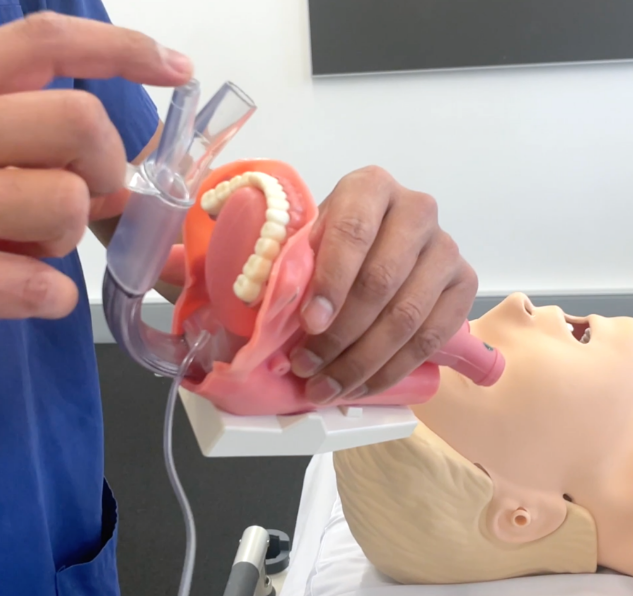
Trauma patients can present with heavily soiled airways often with blood, vomit or foreign bodies. Temporising measures may include suctioning, turning the patient lateral and allowing the patient to assume the position of greatest comfort. However, the gold standard for airway protection remains a cuffed endotracheal tube. It is essential to have at least 2 large bore suction catheters prepared when managing these patients.
In the instance that debris in the airway accumulates as soon as suction is removed, the suction assisted laryngoscopy and decontamination (SALAD) technique may be appropriate.
SALAD
-
The suction catheter clears the oropharynx and glottis of debris.
-
In the case of active regurgitation, the catheter is held in a fixed position on the left side of the laryngoscope, directly in the oesophagus to maintain continuous suction throughout the intubation process.
-
The disadvantage of continuous suctioning can include suctioning of oxygen enriched air.
Supra-Glottic Airway Device (SAD)/ Laryngeal Mask Airways (LMA)
-
The use of LMAs may aid in oxygenation as well as to tamponade bleeding from the upper airway.
-
Second generation LMAs have the added advantages of having higher pressure seals and ports for nasogastric insertion.
-
The Intubating LMAs are designed to allow a flexible endoscope to pass through the LMA and allow for rail–roading of an endotracheal tube.
-
The disadvantage of these devices is that they require adequate mouth opening and may not function with deformed anatomy.
Special patient groups
Traumatic brain injury (TBI)
Managing the airway in patients with TBI presents a dual challenge: protecting the airway while minimising secondary brain injury.
Core priorities include:
-
Maintaining oxygenation: Preventing hypoxaemia and hypotension, as these exacerbate cerebral ischaemia. Effective preoxygenation/apnoeic oxygenation can be crucial in avoiding peri-intubation hypoxaemia.
-
Avoiding cerebral hypoperfusion: Ensure adequate volume resuscitation prior to administering opioids and IV agents which can cause hypotension. Use of an arterial line can be instrumental in ensuring stable peri-intubation haemodynamics.
-
Avoiding raised Intracranial Pressure (ICP): Reverse Trendelenburg positioning can assist in reducing intracranial pressure and facilitating intubation. Adequate analgesia eg: fentanyl 1.5 mcg/kg or IV lignocaine 1.5mg/kg, and use of video assisted laryngoscope limits ICP surges during intubation. Rocuronium is the preferred agent for RSI in TBI as suxamethonium can cause a transient increase in ICP
-
Post-intubation care: Patients should remain well sedated to lower cerebral metabolic demands and prevent seizure due to TBI. Avoid tight-fitting collars and ties or positions that impede venous outflow from the head which can increase ICP.
Facial fractures
Challenges and Risks
-
Facial fractures are often high-energy injuries accompanied by bleeding, swelling, and airway obstruction.
-
Structural instability, such as malocclusion or posterior displacement of fractured segments, can further obstruct the airway.
-
Soft tissue injuries, haematomas, and foreign objects (e.g., teeth or bone fragments) complicate visualisation and access during intubation.
-
The risk of aspiration from blood and secretions is heightened, demanding urgent and effective airway management.
Le Fort Classification
The Le Fort classification provides a systematic approach to describing maxillary fractures, based on their severity and anatomical disruption:
Le Fort I: Horizontal fracture separating the maxilla and palate from the midface. Patients may present with dental misalignment or mobility of the upper teeth.
Le Fort II: Pyramidal fracture extending superiorly through the maxilla, involving the nasal and orbital regions. Often results in swelling, bruising, and midface instability.
Le Fort III: Craniofacial disjunction, where the facial skeleton is entirely separated from the cranium. It is often accompanied by dural tears, cerebrospinal fluid rhinorrhoea, and skull base fractures, complicating airway management further.
Examination and Initial Steps
-
Assess for stridor, hoarseness, and visible deformities. Stridor suggests airway narrowing, requiring immediate action.
-
Suction blood and debris to maintain airway patency.
-
Use Magill forceps as necessary to remove larger foreign bodies.
-
Maintain neutral cervical spine alignment using MILS if indicated.
Techniques for Airway Management
-
Positioning: Patients with unstable midface fractures often prefer sitting upright, as this allows the fractured segment to fall forward, relieving obstruction.
-
Adjuncts: Nasopharyngeal airways may be contraindicated due to potential base-of-skull fractures.
-
Video Laryngoscopy: Preferred for intubation as it enhances visibility without requiring excessive neck extension.
-
Backup Surgical Access: ENT or maxillofacial surgeons should be available for emergency front-of-neck access or other advanced techniques in cases of intubation failure.
Strategies for Intubation
-
Plan for a failed intubation, involving a multidisciplinary team. Ensure all necessary equipment, including a bougie and hyper-angulated video laryngoscope, is ready.
-
In alert, compliant patients, consider awake fibreoptic intubation to maintain spontaneous ventilation during airway visualization.
-
For severe cases, advanced techniques such as retromolar or submental intubation may be required, and these should be performed in a controlled setting ideally in theatre.
Burns
Airway burns and inhalation injuries present significant risks and require close monitoring for signs of deterioration.
Challenges and Risks
-
-
Rapid progression of airway oedema, particularly after fluid resuscitation.
-
Obstruction from ulceration, soot, and secretions can lead to difficult mask ventilation.
-
Hypoxaemia can be caused by pulmonary injury, carbon monoxide poisoning, or compromised lung compliance.
-
-
Delaying intubation can increase difficulty due to progressive swelling and anatomical distortion.
Signs of Airway Injury
-
-
Stridor, hoarseness, and deep burns to the face or neck.
-
Soot or blackened secretions in the oropharynx, singed nasal hairs, or visible swelling.
-
-
-
FNE is a useful tool in predicting airway compromise by oedema or burns. It is well tolerated and is strongly predictive for the need for intubation and allows targeted decision-making.
-
Equipment and Techniques
-
-
ETT: Use a tube with an internal diameter of ≥8 mm to facilitate pulmonary toilet and bronchoscopy for debris and secretion management.
-
-
-
Rocuronium is the preferred NMB for intubation. Suxamethonium is considered safe in the first 24 hours after a burn injury. However, after 24-48 hours there is increased risk of hyperkalaemia with suxamethonium due to upregulation of nicotinic acetylcholine receptors at the neuromuscular junction.
-
Scenario
As the trauma team assembles, roles are assigned, and the necessary equipment is meticulously prepared. You prepare for intubation as your ED colleague administers midazolam, 2mg, ketamine 1mg/kg and rocuronium 1.2mg/kg with metaraminol ready. Your airway assistant prepares for MILS while 2 large suction devices are double checked in anticipation.
Blood and secretions obscure the view. Large-bore suction is deployed, but the airway remains heavily soiled. You adopt the SALAD technique clearing the oropharynx and maintaining a satisfactory view.
Using a hyperangulated video laryngoscope, you avoid unnecessary cervical movements. The first-pass intubation is a success, the endotracheal tube sliding into place with chest rise and fall, misting, ausculatation of breath sounds bilaterally and convincing etCO2 trace for 5 breaths.
The team exhales as the ventilator begins its rhythmic hum. Imaging confirms significant facial fractures, but the airway is secure. You take a step back with the immediate crisis resolved. With the patient’s airway stable and ventilation assured, the team transitions to the next phase of trauma management.

Key lessons in trauma airway management include
-
Thorough preparation and assessment are key.
-
Having the requisite equipment and expert personnel available ensures that unexpected problems are addressed in an appropriate and efficient manner.
-
Special patient populations demand tailored strategies and vigilant monitoring.
-
Airway management in trauma requires excellent teamwork and communication skills.
Athanassoglou V, Rogers A, Hofmeyr R. In-hospital management of the airway in trauma. BJA Educ. 2024;24(7):238-44. Available from: https://www.bjaed.org/article/S2058-5349(24)00031-3/fulltext
Australian and New Zealand College of Anaesthetists (ANZCA) (2016) Airway Assessment Resource. Melbourne: ANZCA. Available at: https://www.anzca.edu.au/getattachment/eff1ab5d-46cf-46db-95ef-5e65ecb88c26/PU-Airway-Assessment-20160916v1
Baratloo A, Ahmadzadeh K, Forouzanfar MM, Yousefifard M, Farhang Ranjbar M, Hashemi B, et al. NEXUS vs. Canadian C-Spine Rule (CCR) in Predicting Cervical Spine Injuries; a Systematic Review and Meta-analysis. Arch Acad Emerg Med. 2023;11(1):e66.
Derakhshan P, Nikoubakht N, Alimian M, Mohammadi S. Relationship Between Airway Examination with LEMON Criteria and Difficulty of Tracheal Intubation with IDS Criteria. Anesth Pain Med. 2023;13(6):e142921.
DuCanto J, Serrano KD, Thompson RJ. Novel Airway Training Tool that Simulates Vomiting: Suction-Assisted Laryngoscopy Assisted Decontamination (SALAD) System. West J Emerg Med. 2017;18(1):117-20.
Kelly FE, Frerk C, Bailey CR, Cook TM, Ferguson K, Flin R, et al. Implementing human factors in anaesthesia: guidance for clinicians, departments and hospitals: Guidelines from the Difficult Airway Society and the Association of Anaesthetists: Guidelines from the Difficult Airway Society and the Association of Anaesthetists. Anaesthesia. 2023;78(4):458-78.
McCann C, Watson A, Barnes D. Major burns: Part 1. Epidemiology, pathophysiology and initial management. BJA Educ. 2022;22(3):94-103.
Park L, Zeng I, Brainard A. Systematic review and meta-analysis of first-pass success rates in emergency department intubation: Creating a benchmark for emergency airway care. Emerg Med Australas. 2017;29(1):40-7.
Russotto V, Myatra SN, Laffey JG, Tassistro E, Antolini L, Bauer P, et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA. 2021;325(12):1164-72.
Saini S, Singhal S, Prakash S. Airway management in maxillofacial trauma. J Anaesthesiol Clin Pharmacol. 2021;37(3):319-27.
Ultrasonography measurement of glottic transverse diameter and subglottic diameter to predict endotracheal tube size in children: a prospective cohort study. Scientific Reports, 12(1).