By Dr. Anei Ochan-Thou, Dr. Zheng Cheng Zhu, Dr. Nicola Wevling, Dr. Lahiru Amaratunge.
In our last article, we were tangled up in the brachial plexus. This time, we are looking at the lumbosacral plexus, a close cousin of the brachial plexus. In a similar vein, the lumbosacral plexus provides motor and sensory supply to the lower limb.
In this article, we will be looking at the anatomy and function of the main terminal branches of the lumbosacral plexus. This will set the backdrop for an article series on regional anaesthesia blocks. Knowing our anatomy for regional blocks helps us to locate the appropriate landmarks for anaesthetic injection.
The Lumbosacral Plexus

Figure 1. Schematic of the lumbosacral plexus, demonstrating relationship of nerve roots, divisions, and terminal branches.
Imagine a busy switchboard connecting calls between your spine and lower limbs. That’s the lumbar and the sacral plexi. Thanks to the lumbosacral trunk (the middleman), there is substantial overlap between the lumbar and sacral plexus, so much so that they are often collectively referred to as the lumbosacral plexus. This networking hub is formed from the ventral rami of L2-S3, making up the motor and cutaneous supply of our lower limbs.
The lumbar component of the lumbosacral plexus, originating from L1-L4, exits the spinal canal through the intervertebral foramen and enters into the psoas major muscle. Within this muscle, the roots split into the anterior and posterior divisions, reuniting to form the individual nerves of the lumbar plexus. Think of it as a nerve-themed family tree! (See image below which shows the branches of the lumbar plexus)
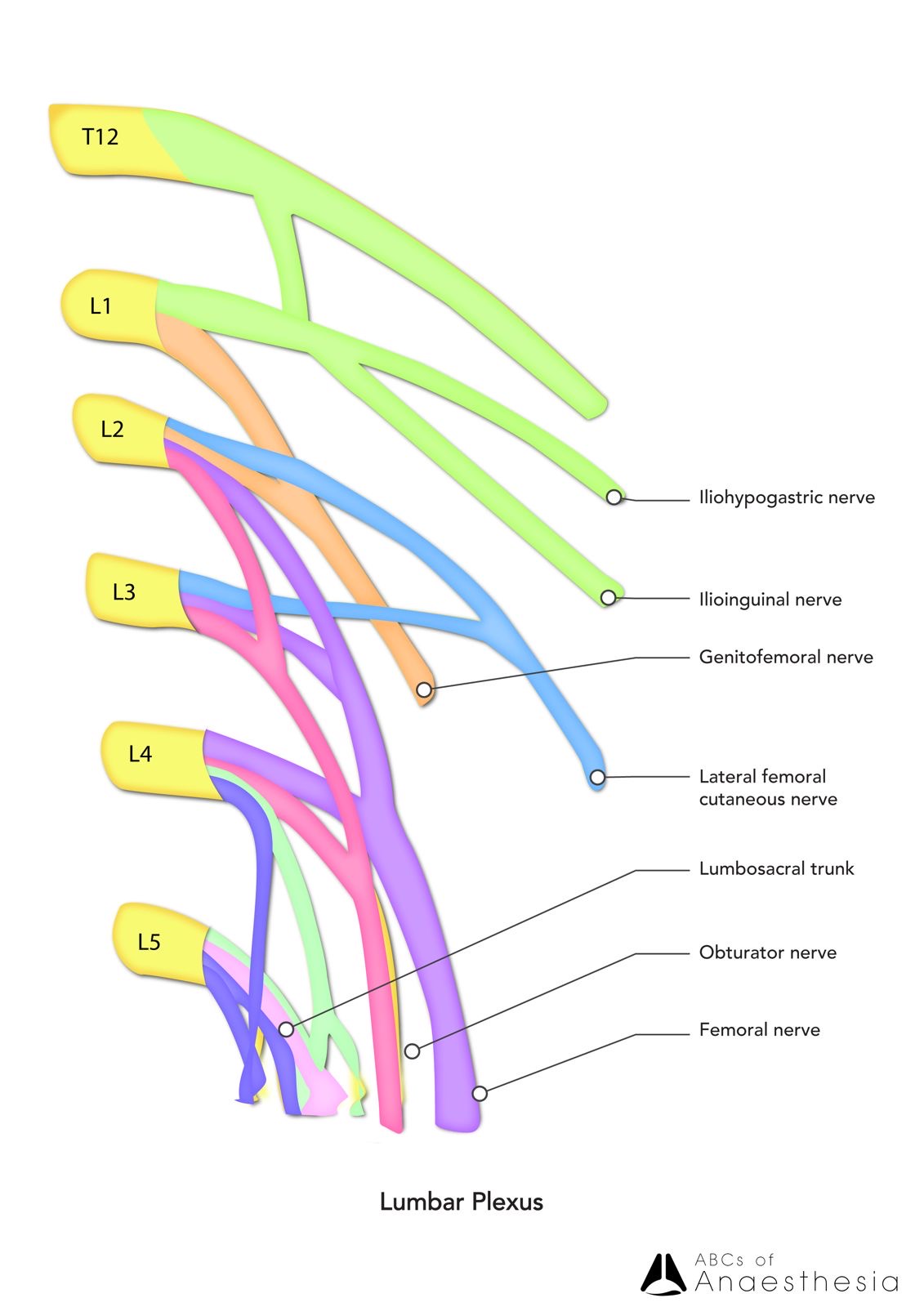
Figure 2. Close-up schematic of the lumbar component of the lumbosacral plexus
The sacral component of the lumbosacral plexus arises from the spinal nerves L4-S4, with some fibres from the lumbar plexus. Among these nerves, the largest is the sciatic nerve, comprising the common peroneal/fibular nerve and the tibial nerve, wrapped in a common sheath.
Due to its relatively deep location, the lumbosacral plexus is protected from acquired injuries. However, temporary deficiencies/ lesions may occur in the setting of pregnancy and childbirth, retroperitoneal pathology, and pelvic malignancies
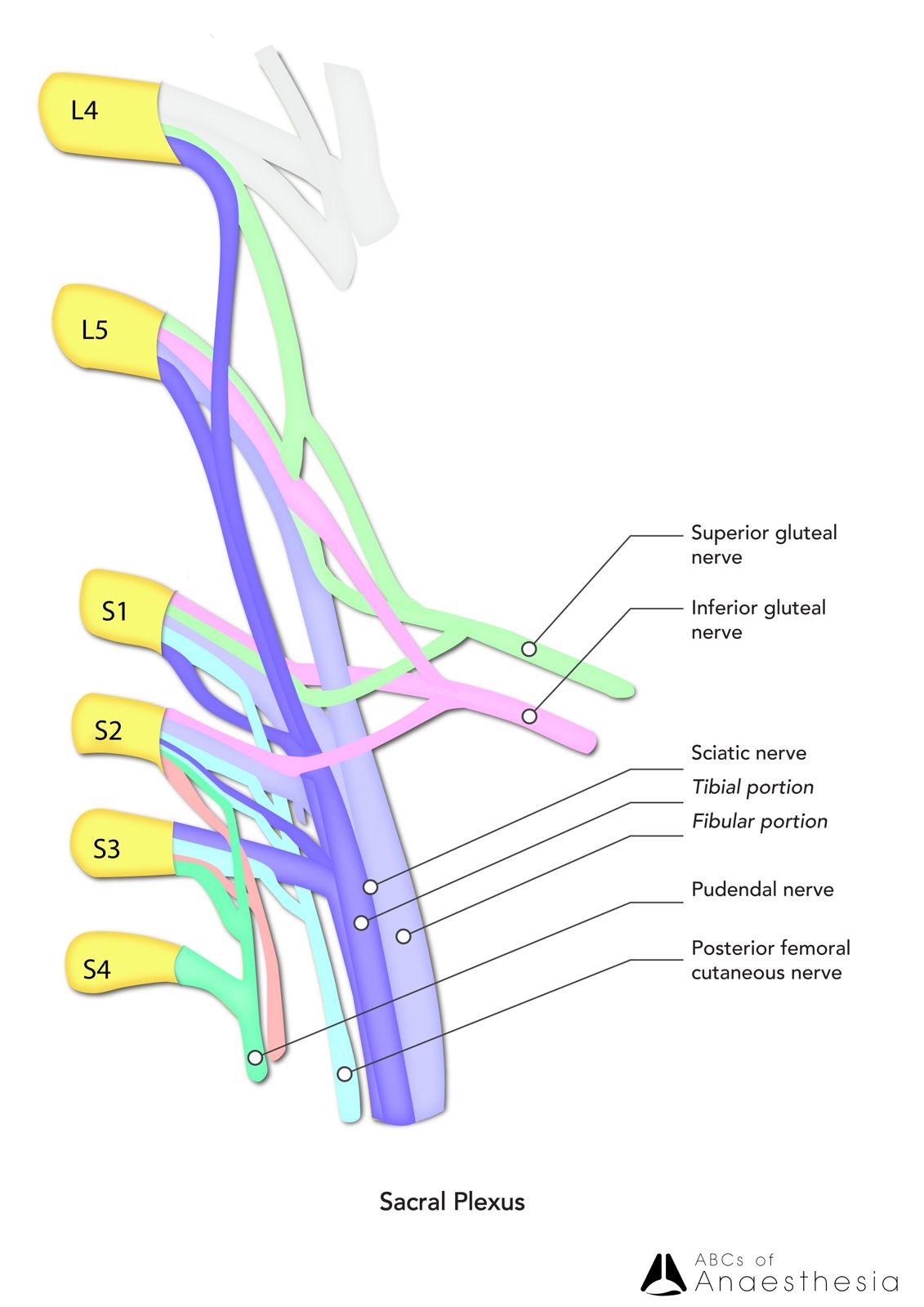
Figure 3. Close-up schematic of the sacral component of the lumbosacral plexus. Note the close association of the two major terminal branches in forming the sciatic nerve: the common peroneal nerve (AKA common fibular nerve) and the tibial nerve.
Clinically, if there is damage to one of these nerves, the deficiency will be seen within the specific muscles and cutaneous innervation that the nerve supplies. At the spinal nerve level, this is commonly manifested as radiculopathy, which can comprise both positive (such as radicular pain, paraesthesia)and negative symptoms (such as numbness, weakness) that anatomically align with the supplied distribution of the affected nerve or nerve group. One of the most common lumbosacral pathologies is “sciatica”which describes the radicular pain originating from the lower back and hip region, radiating along the posterior thigh in the inferior direction – the very course of the sciatic nerve that is supplied by the lower lumbar and sacral nerve roots.
Additionally, injury of the distal terminal nerve branches can result in peripheral neuropathy with the same positive and negative symptoms and signs. For example, injury to the common fibular nerve, which commonly occurs due to its superficial location at the head and neck of the fibula, results in paresis/paralysis of the anterior and lateral leg muscle compartments, manifesting as foot drop and weakness in ankle eversion. Similarly, injury to the tibial nerve can result in paralysis of the calf muscles, leading to an inability to plantar flex the foot and the development of a shuffling gait.
Now equipped with our knowledge of the anatomy and pathology associated with the lumbosacral plexus, let’s delve a little deeper into the major nerves and their motor and cutaneous innervations.
Femoral nerve (L2-L4): The Overachiever
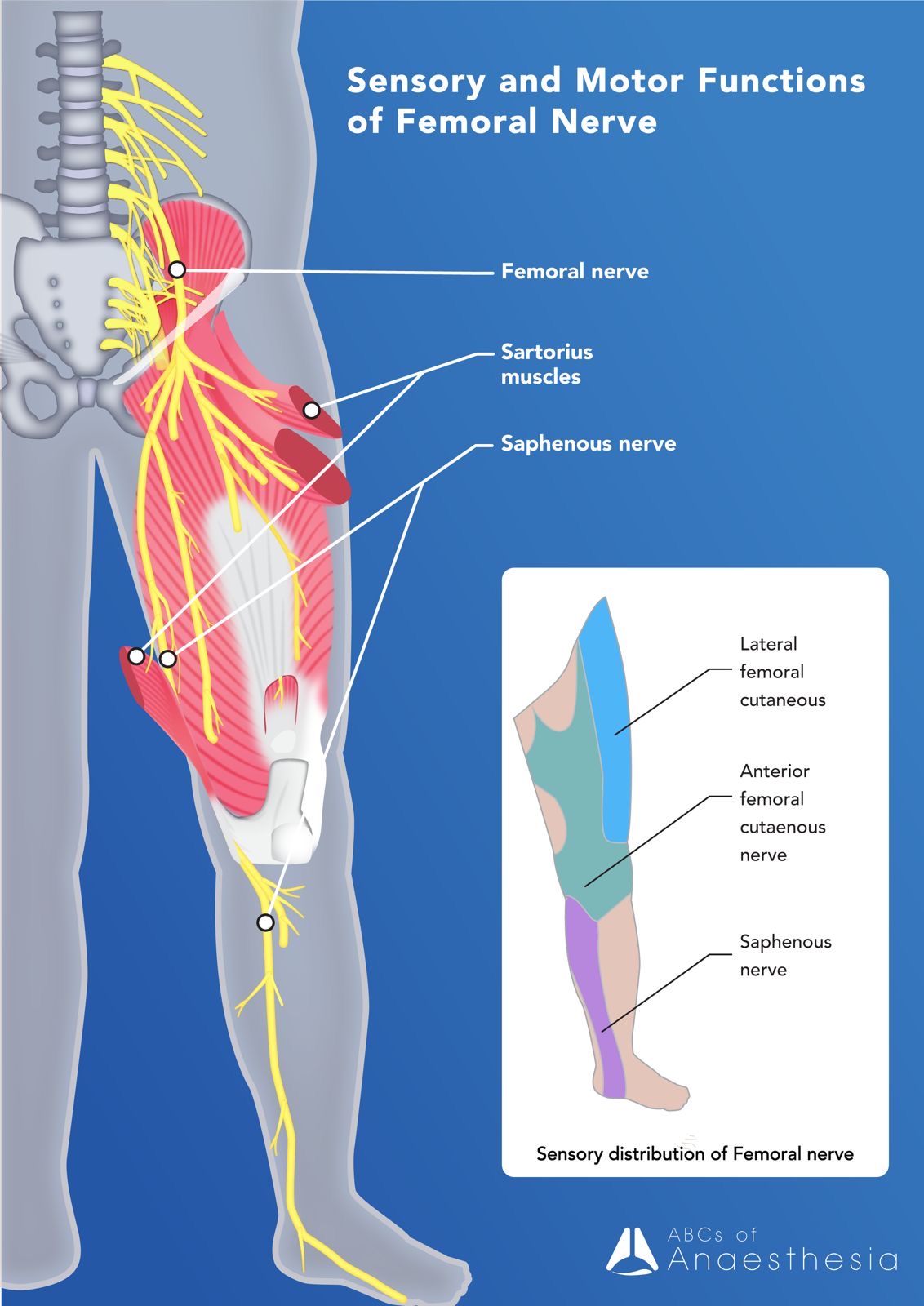
| Course | Originates from the posterior division of the L2-L4 ventral rami
Passes into the thigh below the inguinal ligament into the femoral triangle Deep terminal branch exits the femoral triangle to become the saphenous nerve coursing into the leg via the adductor canal |
| Motor | iliacus, pectineus, quadriceps femoris, sartorius
-> hip flexion, knee extension, external rotation |
| Sensory | Large cutaneous area on the anterior and medial compartments of the thigh, medial leg and foot (saphenous nerve), and gives articular branches to the hip, knee, and ankle |
Obturator nerve (L2-L4): The Quiet Performer
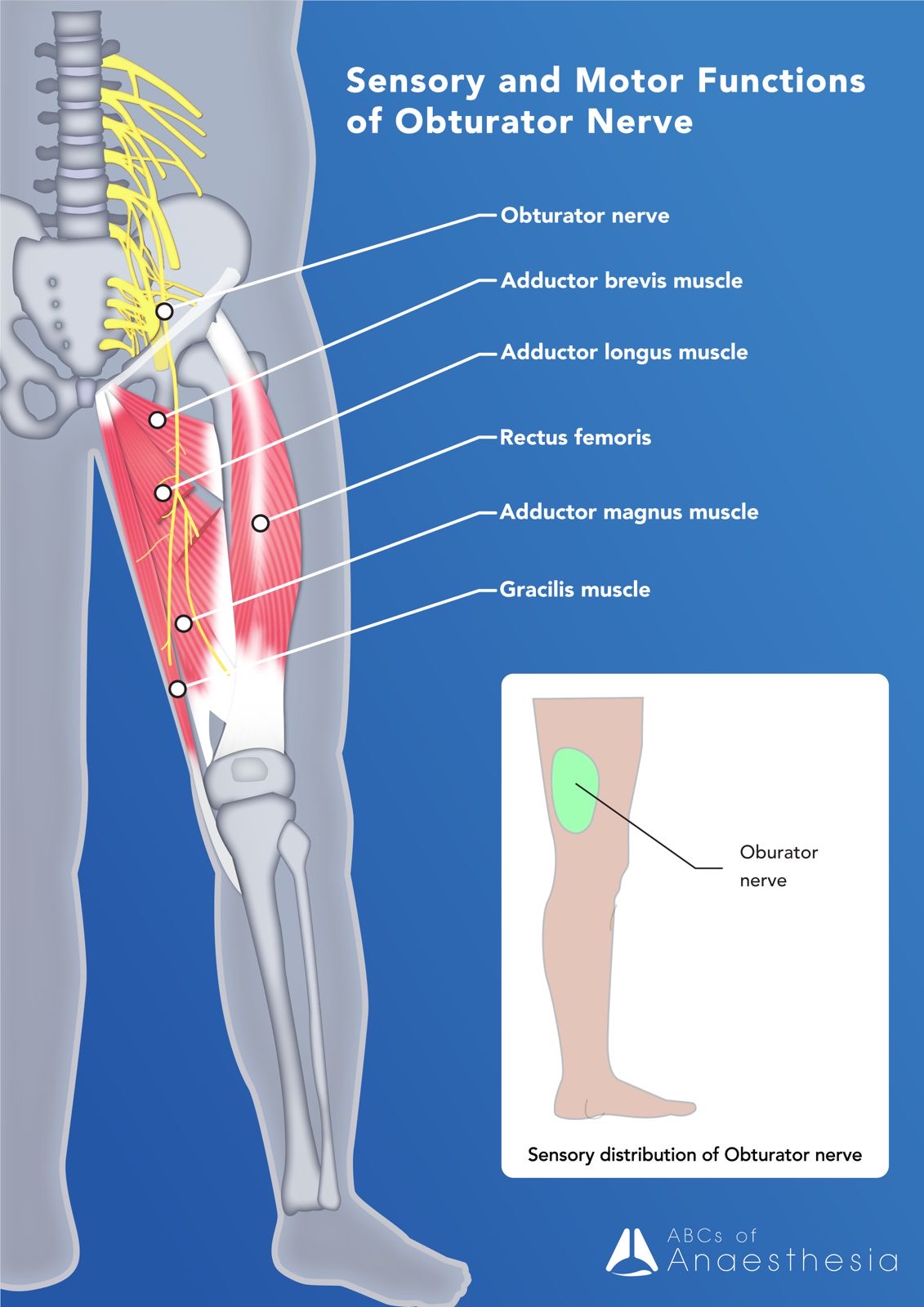
| Course | Originates from the anterior division of the L2-L4 ventral rami
Descends medial to psoas major into the obturator canal and the medial compartment of the thigh |
| Motor | adductor longus, adductor magnus and adductor brevis + gracilis, obturator externus
-> hip adduction |
| Sensory | Medial compartment of the thigh |
Sciatic nerve (L4,L5, S1-3): The Beast
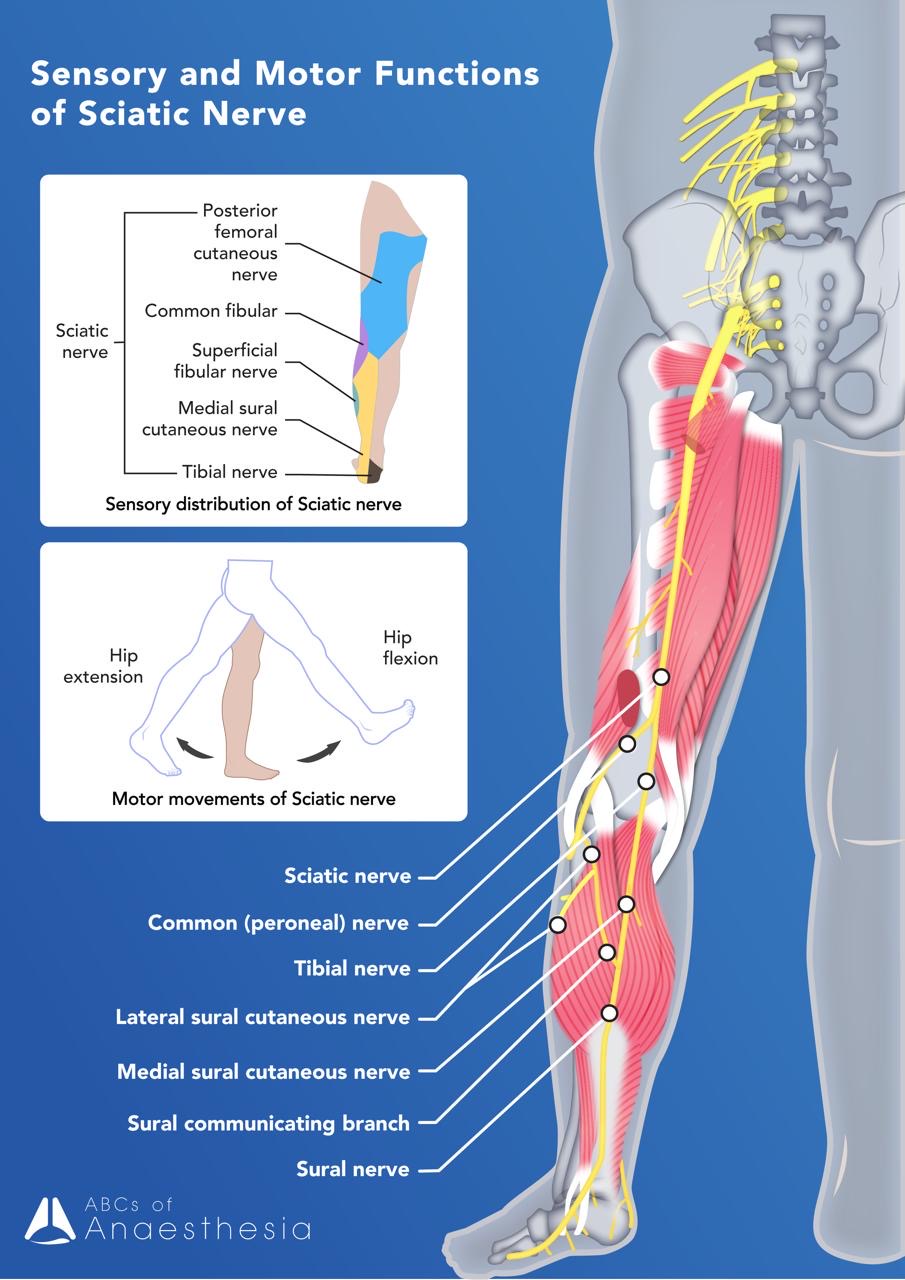
| Course | Originates from S1 to S3, including supply from L4 and L5
Located within a common sheath containing the two major nerves Divides into the tibial and common fibular (peroneal) nerves proximal to the knee – level of bifurcation can be variable |
| Motor | Hamstring muscles (semitendinosus, semimembranosus and biceps femoris) + hamstring part of adductor magnus
-> hip extension, knee flexion |
| Sensory | Anterior division – tibial nerve, sensation: posterior thigh
Posterior division – common peroneal/fibular nerve, sensation: lateral aspect of leg |
Tibial (L4,L5, S1-3): The Reliable Sidekick
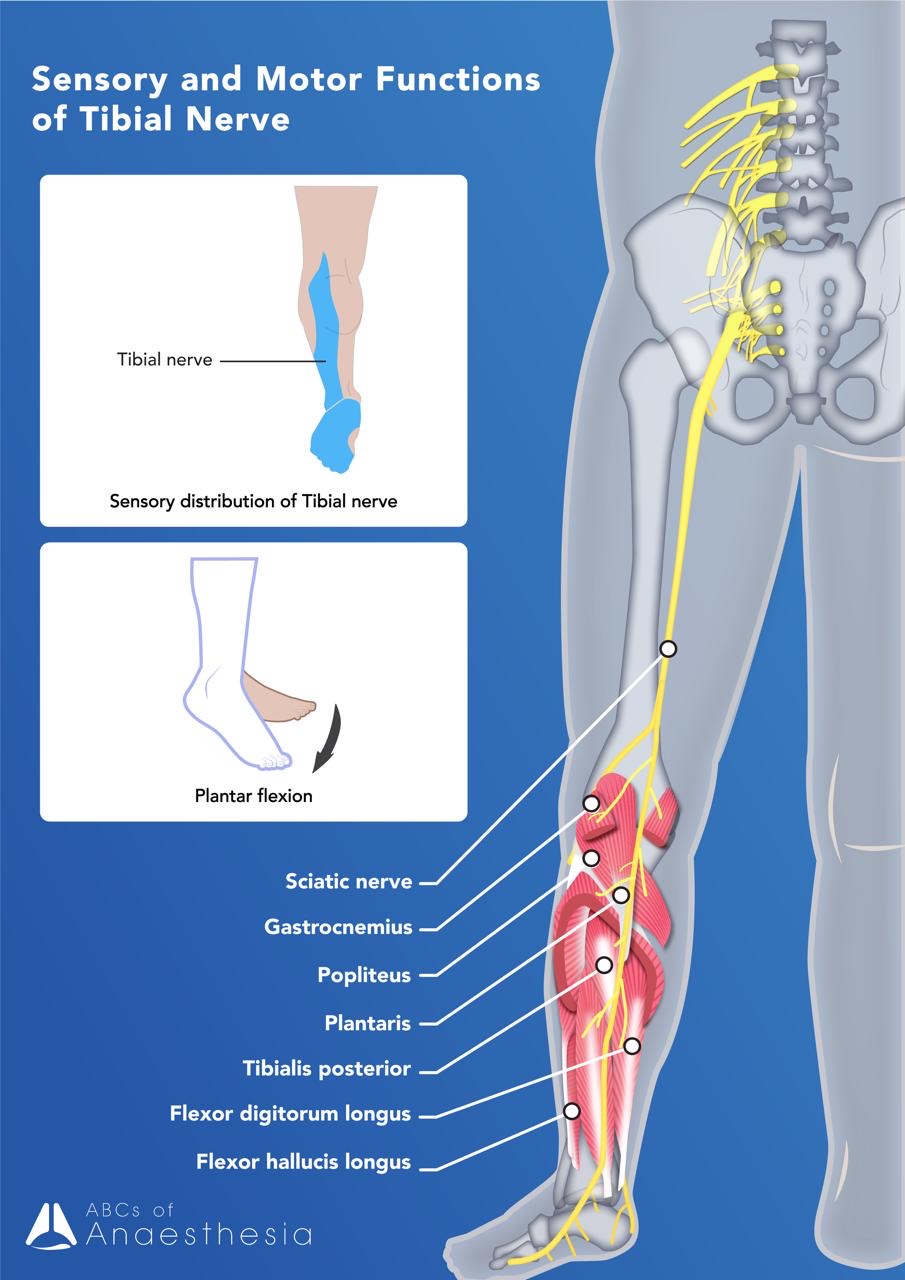
| Course | Supply from anterior divisions of the lumbosacral plexus of the ventral rami of L4-L5, S1-S3
Bifurcates from the sciatic nerve above the knee Courses into the popliteal fossa, deep to gastrocnemius, and under the flexor retinaculum at the ankle
|
| Motor | Muscles within the posterior compartment of the leg (gastrocnemius, soleus, plantaris, toe flexors, popliteus)
-> ankle plantarflexion + inversion, knee flexion/stabilisation, toe flexion |
| Sensory | Posterior compartment of the leg: sural nerve and peroneal communicating nerve
Sole, the lateral border of the foot and the medial and lateral sides of the heel |
Common Fibular Nerve (L4,L5,S1,S2): The Wanderer
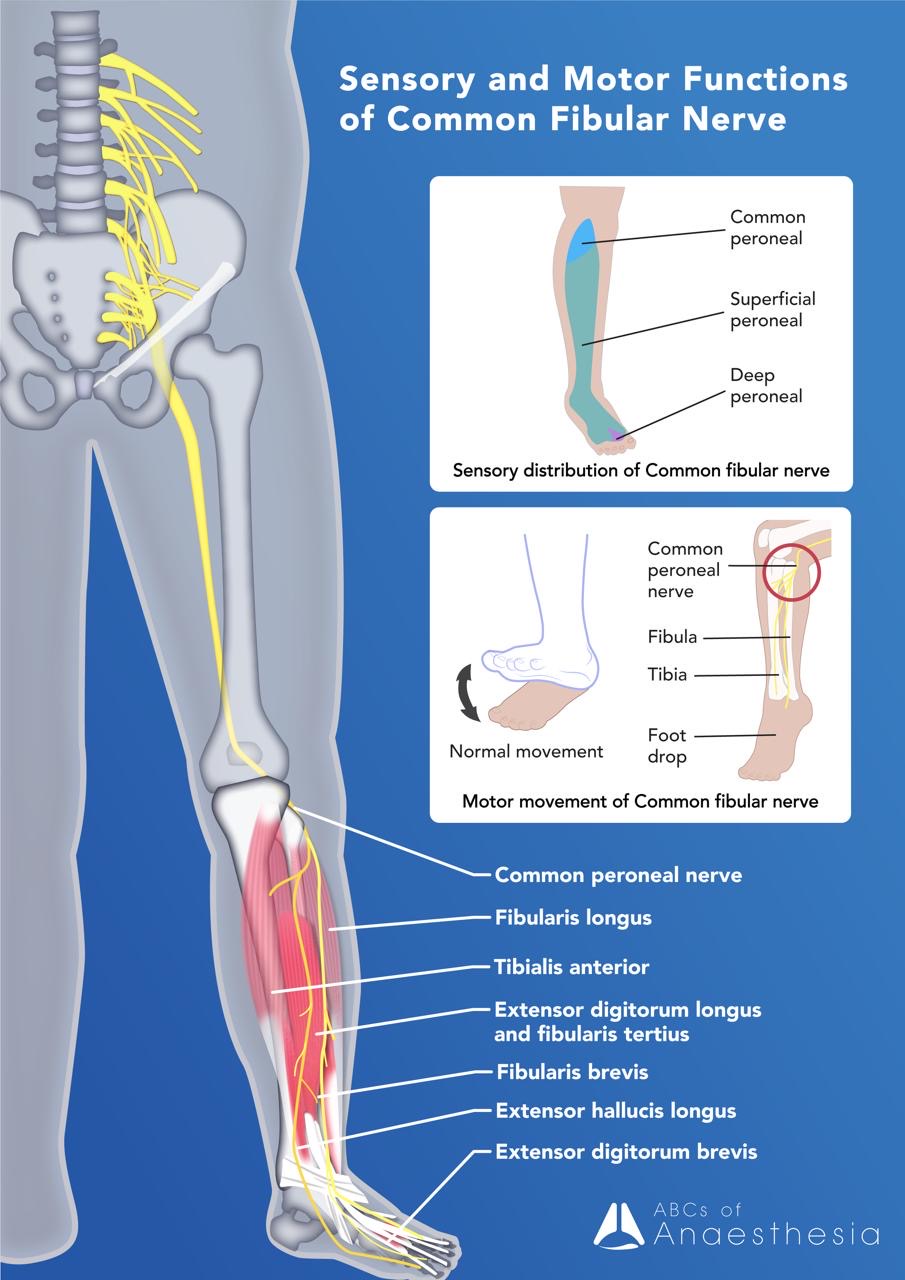
| Course | Supply from posterior divisions of the lumbosacral plexus of the ventral rami of L4-L5, S1-S3
Bifurcates from the sciatic nerve above the knee Winds around the neck of fibula, within the substance of peroneus longus, divides into the terminal branches of the superficial and deep peroneal nerves. |
| Motor | Superficial peroneal nerve: peroneus brevis and peroneus longus
-> foot eversion and ankle plantarflexion Deep peroneal nerve: anterior compartment muscles of the leg -> ankle dorsiflexion |
| Sensory | Superficial peroneal nerve: anterolateral leg and dorsum of the foot
Deep peroneal nerve: cleft between the great and second toes |
Gluteal nerves (L4,L5,S1,S2): The Party Starters.
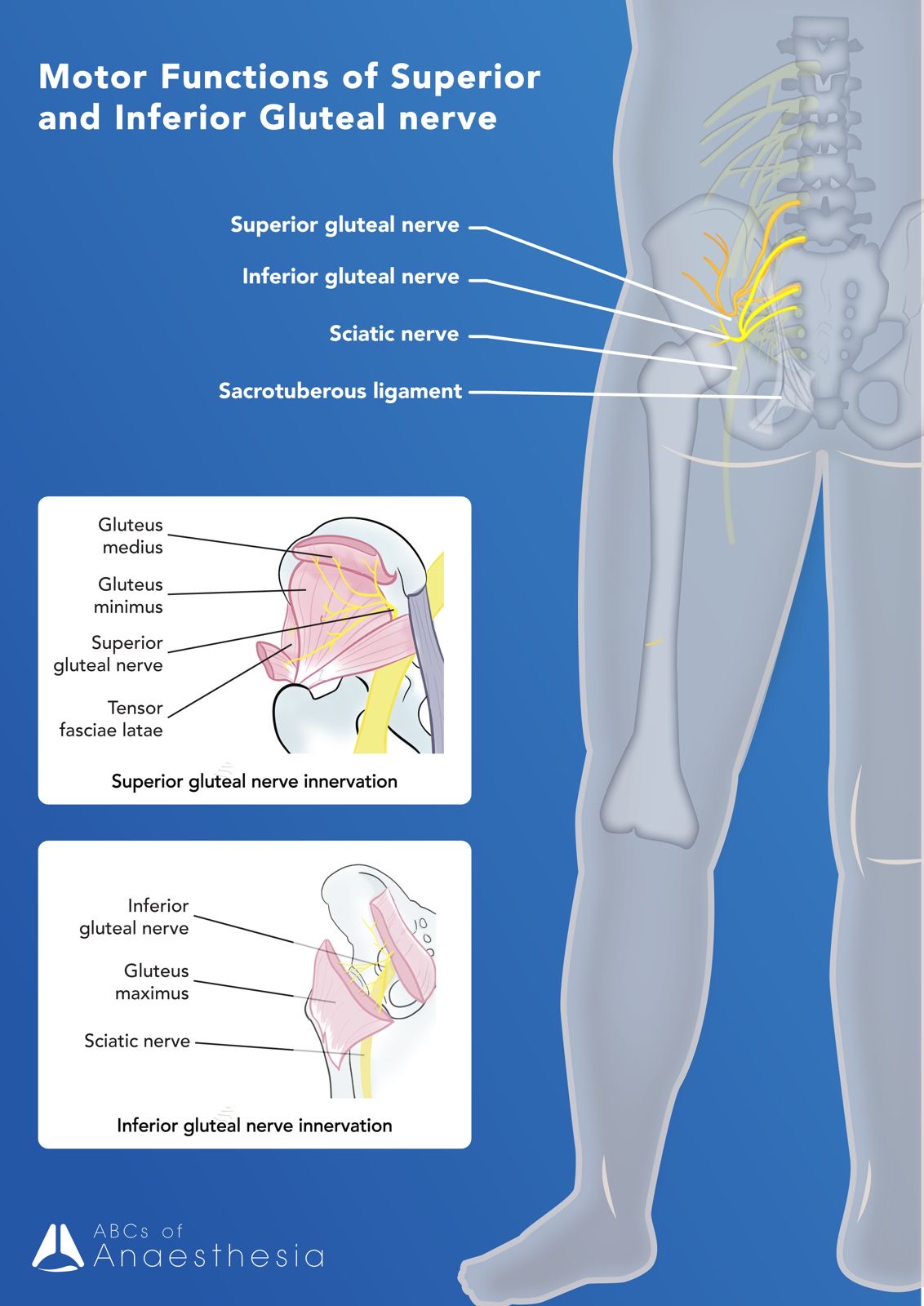
| Course | Superior and inferior gluteal nerves. Originating from the posterior divisions of the lumbosacral plexus.
Both exit the pelvis via the greater sciatic foramen traversing the piriformis muscle (superior gluteal nerve passing over and inferior gluteal nerve passing under) terminating in the gluteal muscles. |
| Motor | Superior gluteal nerve supplies the gluteus medius, gluteus minimus, and the tensor fascia lata
-> Hip abduction and medial rotation Inferior gluteal nerve supplies the gluteus maximus. -> Hip extension and lateral rotation |
| Sensory | Nil |
Pudendal nerve (S2,S3,S4)
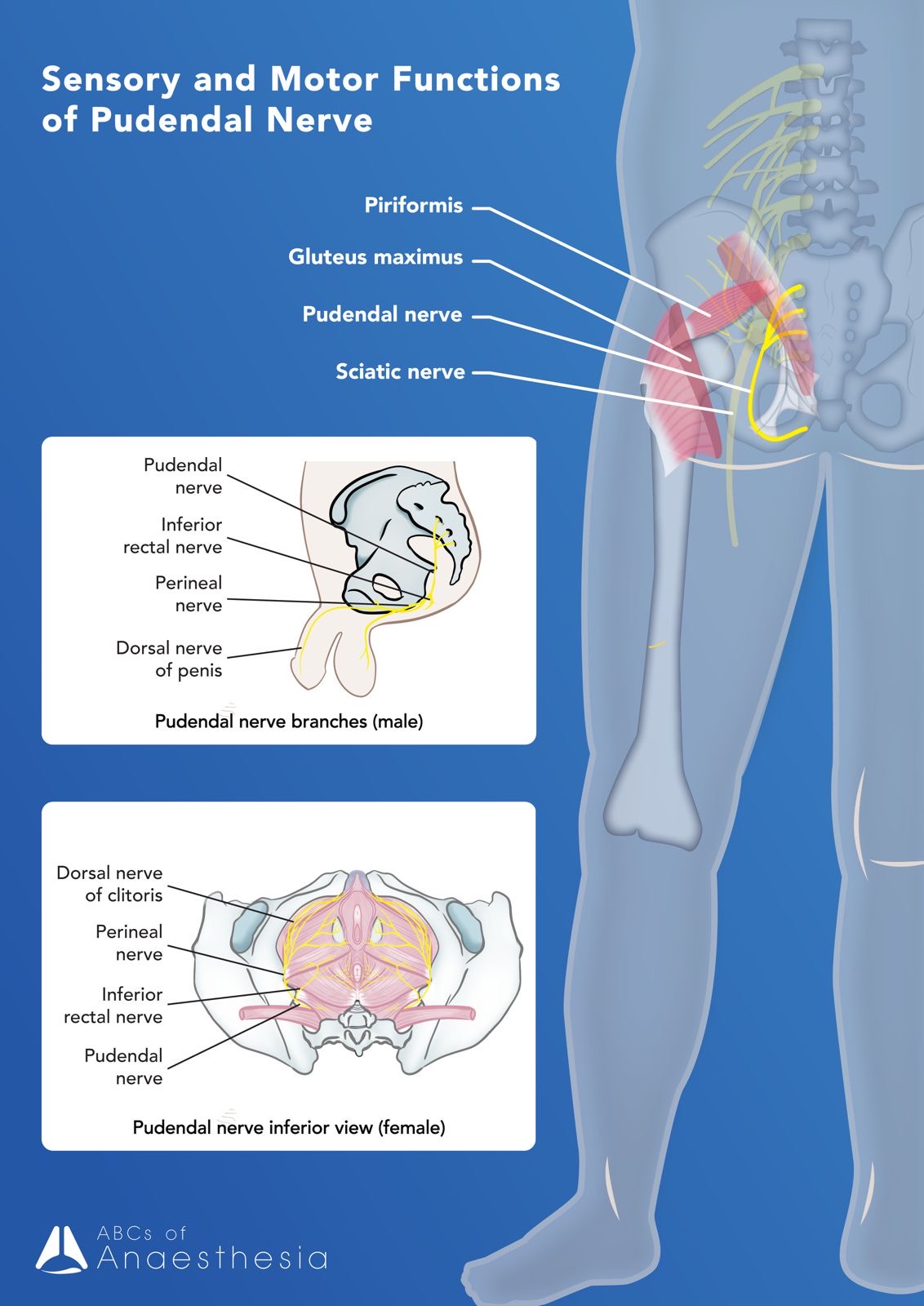
| Course | Principal nerve of the perineum, originating from the anterior divisions of S2, S3 and S4. |
| Motor | Levator ani muscles as well as the external urethral and external anal sphincters.
Important role in continence and pelvic floor stability |
| Sensory | Cutaneous supply to skin around the anus, anal canal, perineum, and external genitalia of both sexes. |
That’s the introduction in the lumbosacral plexus and its anatomy. In our future articles, we will explore how this anatomy assists with lower limb regional blocks and the anaesthetic considerations of these blocks.
Keep a look out for them!
References:
Davies, K. (April 26, 2024). Lumbar Plexus. Teach Me Anatomy. https://teachmeanatomy.info/lower-limb/nerves/lumbar-plexus/
Davies, K. (July 8, 2024). The Sacral Plexus. Teach Me Anatomy. https://teachmeanatomy.info/lower-limb/nerves/sacral-plexus/
Palastanga, N., Field, D., & Soames, R. (2006). Anatomy and human movement: structure and function (Vol. 20056). Elsevier Health Sciences.