By Dr. Nam Gupta
Contents
- Overview
- The Grip
- Optimising Bag-mask ventilation (BMV)
Overview
Methods of Oxygenation:
- Bag-mask
- LMA
- ETT
- Surgical Airway
- Other (jet ventilation and high flow)
The 3-axis model:
- Oral axis (perpendicular to the bed)
- Pharyngeal axis (just over 90o to the oral axis)
- Laryngeal axis
The aim of the 3 axis model is to highlight that the aperture to view the larynx and ventilate the lungs through an open mouth/nose is difficult unless the 3 axes are aligned. This is achieved through
- Positioning (sniffing the morning air, atlanto-occipital extension and lower c-spine flexion)
- Manoeuvres (jaw thrust, chin lift, head tilt)
- Adjuncts and instruments (laryngoscope, Guedel’s airway)
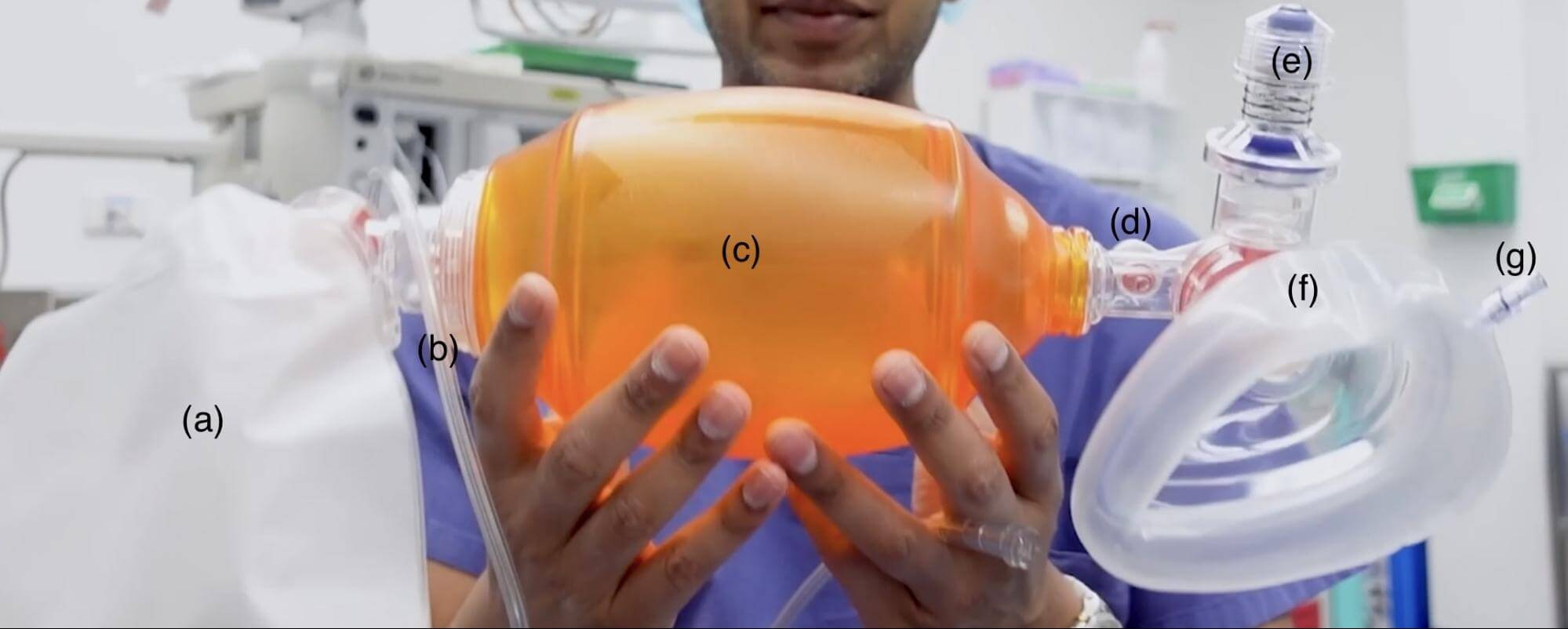
BMV apparatus:
The BMV apparatus is a self-inflating resuscitation system. Common models found around the hospital are the AmbuTM(orange bag) and LaerdalTM (yellow bag).
- PEEP valve: titrate 5-15 cmH2O, delivers PEEP which improves oxygenation
- Self-inflating bag: adult size is around 2L in capacity, aim to deliver around 6-8 ml/kg tidal volume
- O2 bag: ensure attached to O2 supply and inflated
a) O2 reservoir
b) O2 tubing
c) Self-inflating bag
d) Pop-off valve
e) PEEP valve
f) Mask
g) Cuff to inflate mask

a) Squeeze bag ⅓ with one hand = 500ml, slow and small squeeze over 1-2s, 12 breaths/min
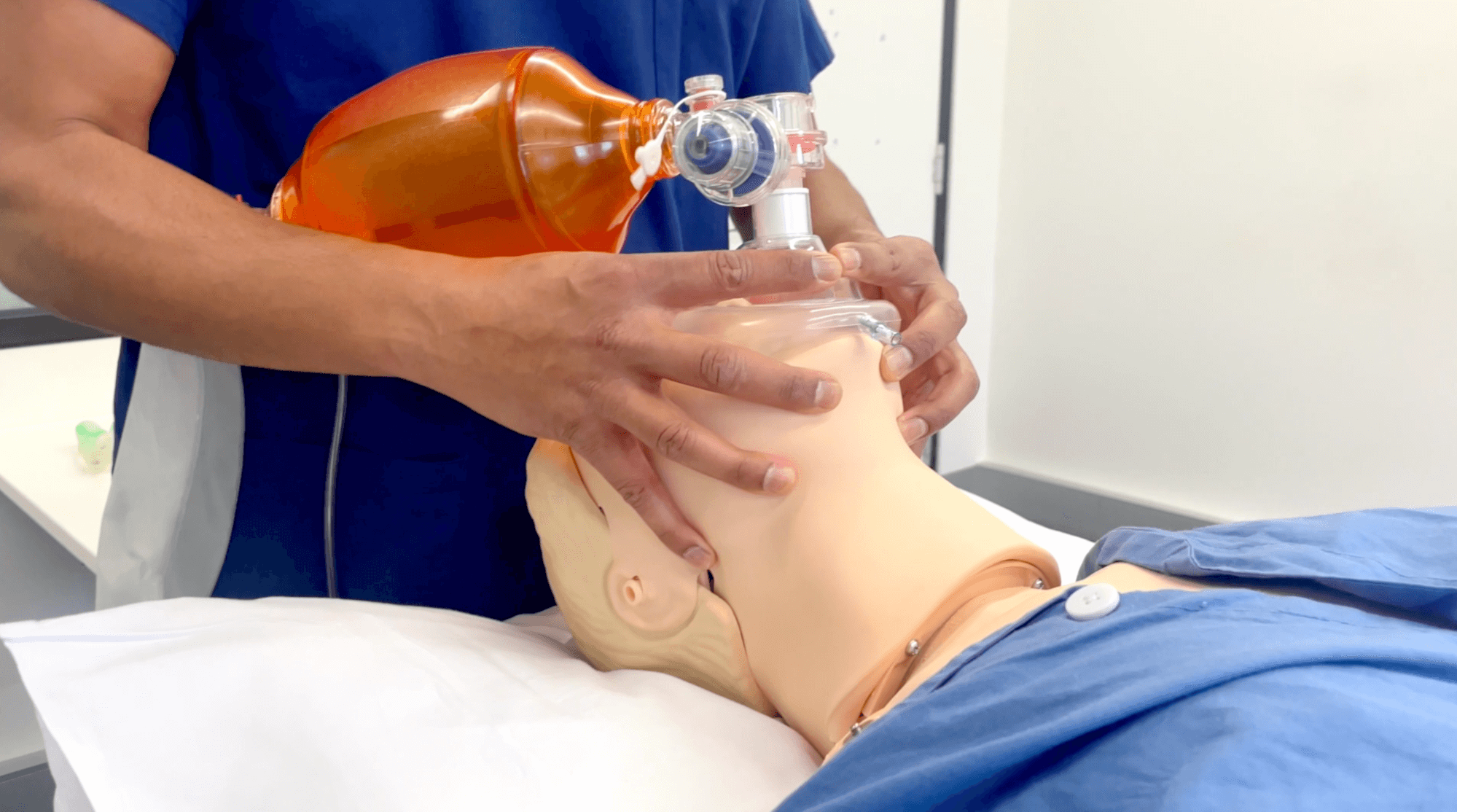
The Grip
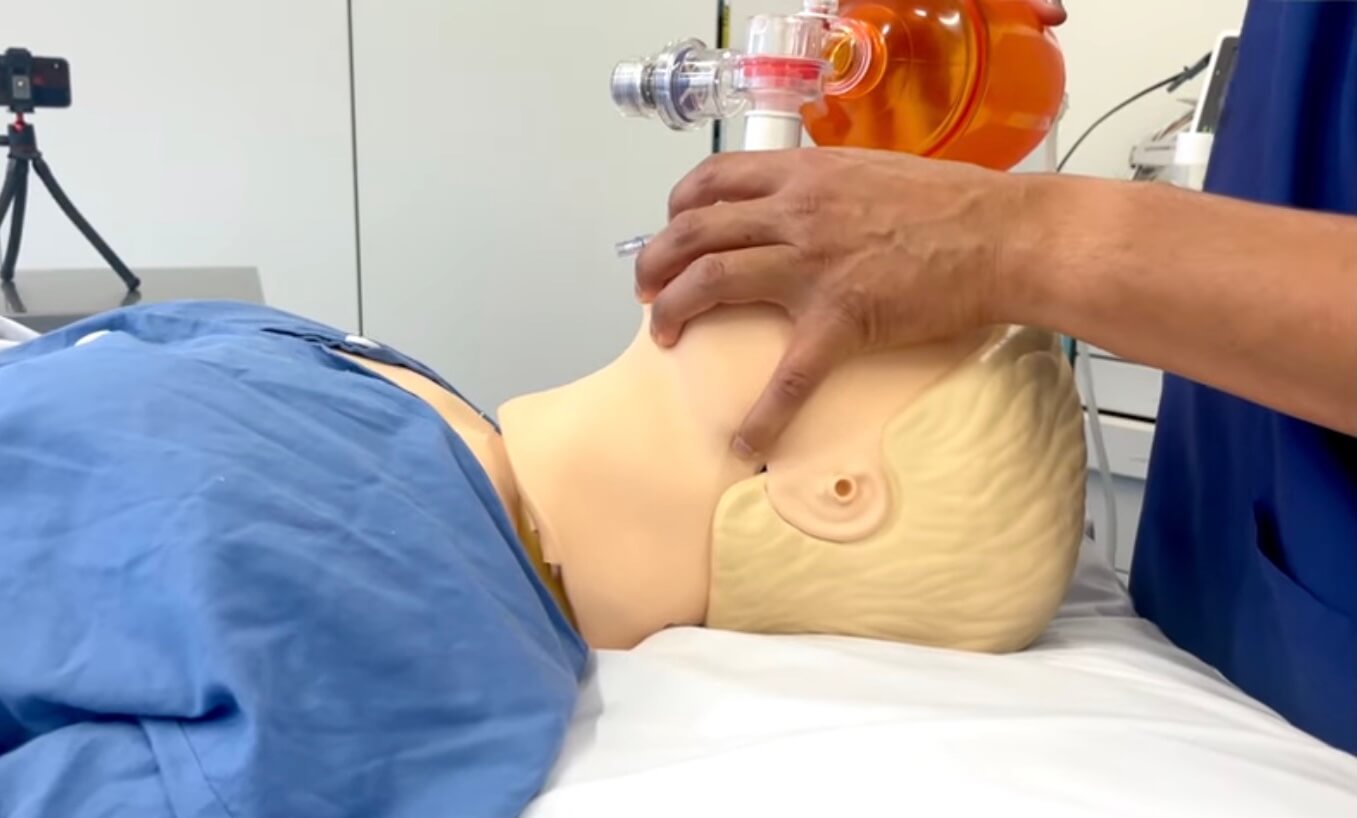
The CE Grip
- C-grip (gentle pressure down)
- Thumb: over the nasal/pointy part of the mask
- 2nd finger: over the flatter part of the mask
- E-grip (over the bony part of the mandible, not the soft tissue)
- 3rd finger: at the chin
- 4th finger: in between along the mandible
- 5th finger: angle of mandible
Tip: The goal is to bring the patient’s face to the mask, rather than pushing the mask down into the patient (makes the oral-pharyngeal/laryngeal angle less acute).
The Two-handed Grips
Require an assistant to bag
The Double CE Grip
- As above but with both hands
- Use when ventilation is difficult (e.g. elderly, not wearing dentures, obstructions, beard etc)
The Vice Grip
- Thenar eminences over the edges of the mask
- The remaining 4 fingers forming the E grip
- Use when smaller hands, weak grip, rescue bag-mask ventilation
Tip: If there is still a leak, ask an assistant to apply pressure over the area causing the leak.

a & b) One-handed CE grip


c) Double CE grip d) Vice grip

e) Bringing the patient’s face to the mask opens the airway f) Pushing the mask down closes the airway
Optimisation of BMV
1. Size
Fitting the mask
- Pointy part – over the nasal bridge
- Flat part – above the mental prominence (dip in between your bottom lip and chin)
Tip: size the mask to fit in between the above two parts, so it does not hang past the chin.
2. Positioning
‘Sniffing’ position – lower C-spine flexion + atlanto-occipital extension
- The tragus of the ear should be in line with the sternal angle
3. Paralysis
You will notice patients are easier to bag once they become paralysed.
NB: this may be a high risk option as the patient cannot breathe on their own. ONLY PERFORM IF YOU ARE A QUALIFIED AIRWAY PRACTITIONER.
4. Manoeuvres (goal is to align the 3 axis)
Jaw thrust
- Lifts soft tissue structures off the oropharynx, allowing easier passage of air
- 1st and 2nd fingers behind the angle of the mandible, then lift
- Put the palms of your hands on the cheeks to get a better grip
- NB: painful in the awake patient
Chin lift
- Place finger over the mental prominence (under the chin) and lift up
- Can be used to maintain the jaw thrust more passively
Head tilt
- Place the top of patient’s head in palm of your hand and tilt along the atlanto-occipital axis (like exaggerating the ‘sniffing’ position)
- Aligns the oral and pharyngeal/laryngeal axis
- Also useful when intubating or inserting LMA
- NB: do not perform on patients with unstable neck injuries (eg trauma, severe rheumatoid arthritis of the neck)
Combination
- Jaw thrust + opening mouth (advanced)
-
- Sweep the tongue off the upper palate

a & b) Jaw thrust
c) Chin lift
d) Head tilt – LMA and laryngoscope
5. Adjuncts
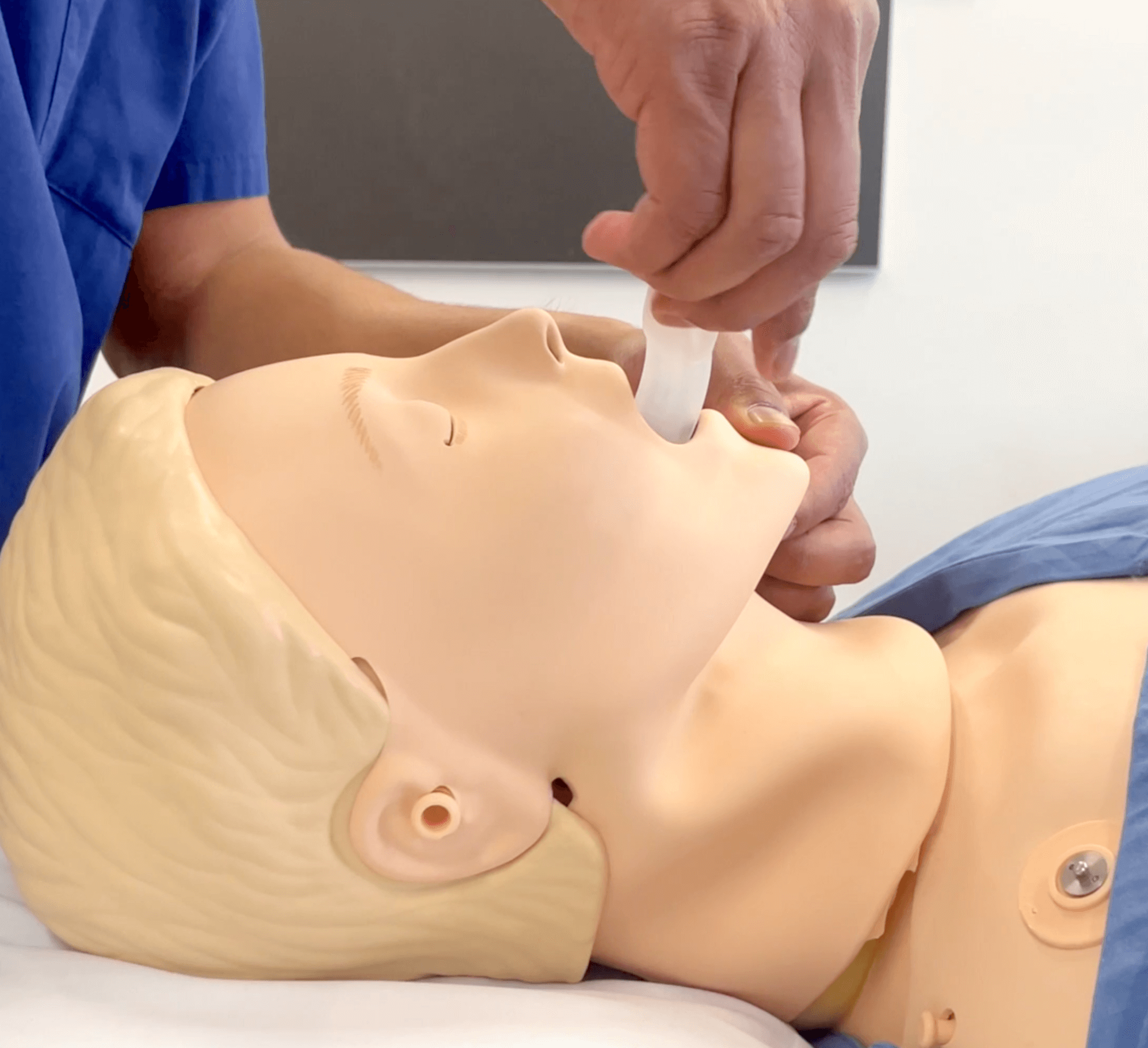
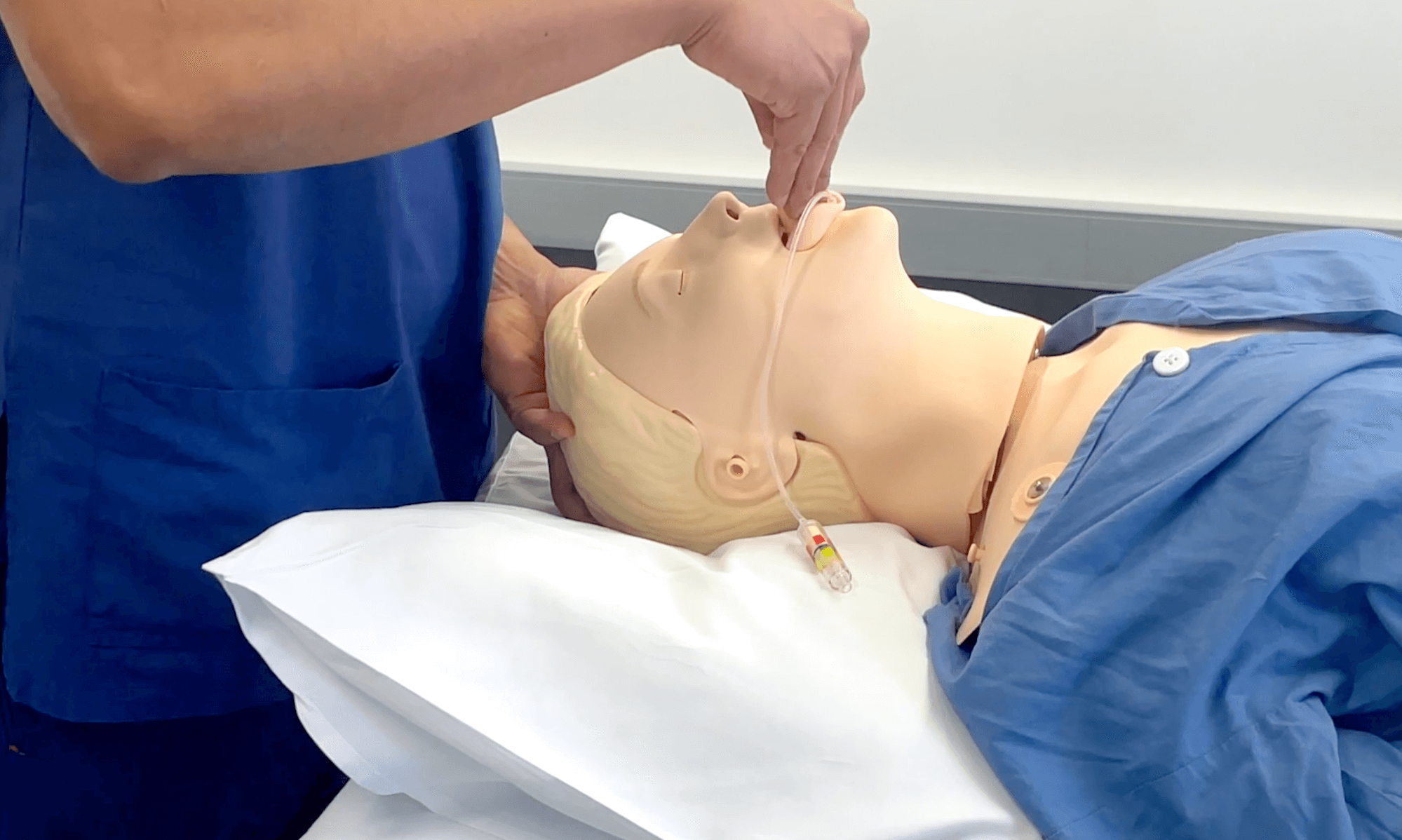
Nasopharyngeal
- Use co-phenylcaine spray (mitigate risk of epistaxis and pain) and lubricant
- Sizing: tip of nose -> earlobe (where it sits in the nose)
- Insertion: insert at 90o angle to the patient
- Caution in patients on anticoagulation, may be contraindicated in head trauma/base of skull fracture
a) Nasopharyngeal airway
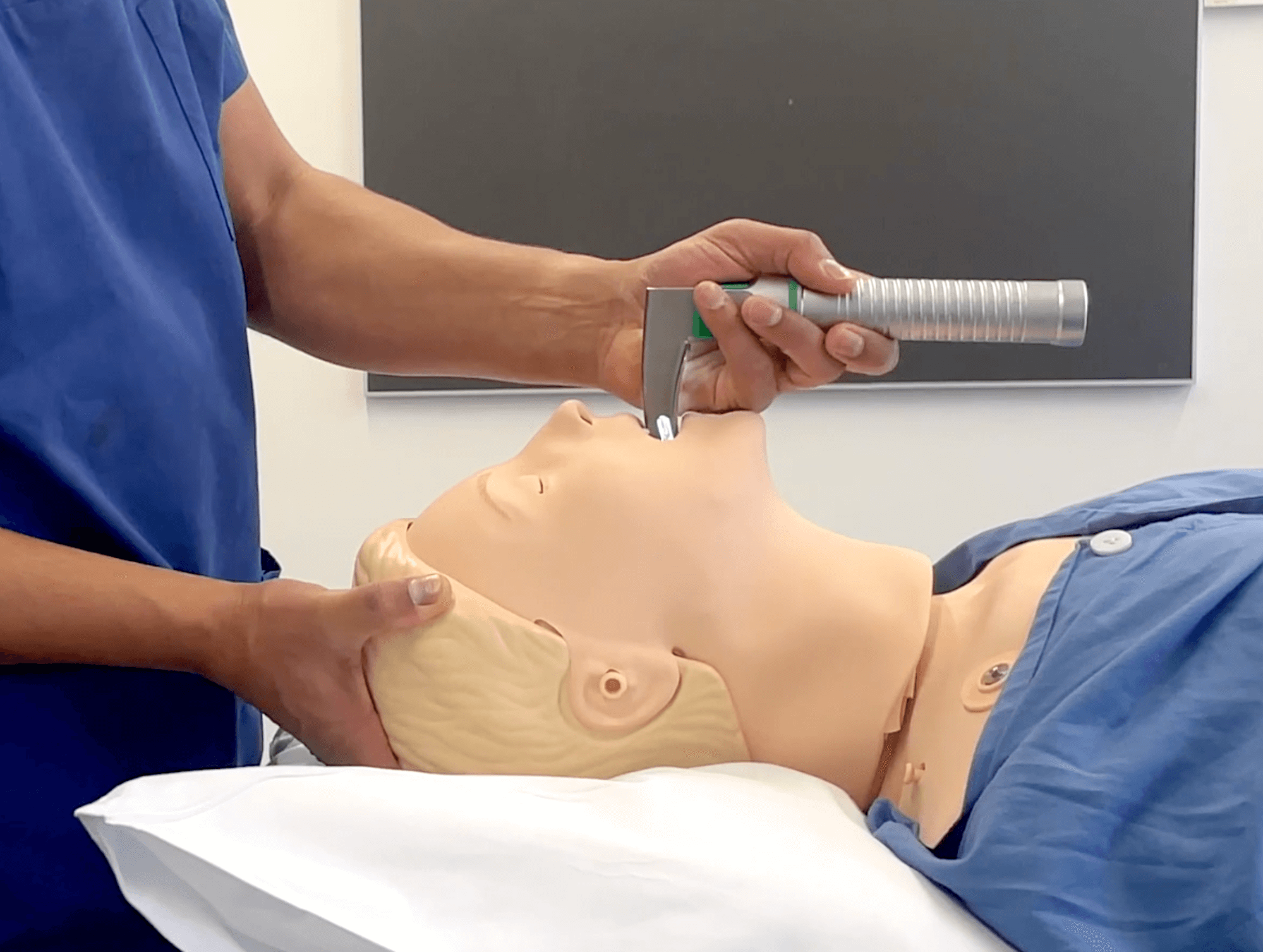
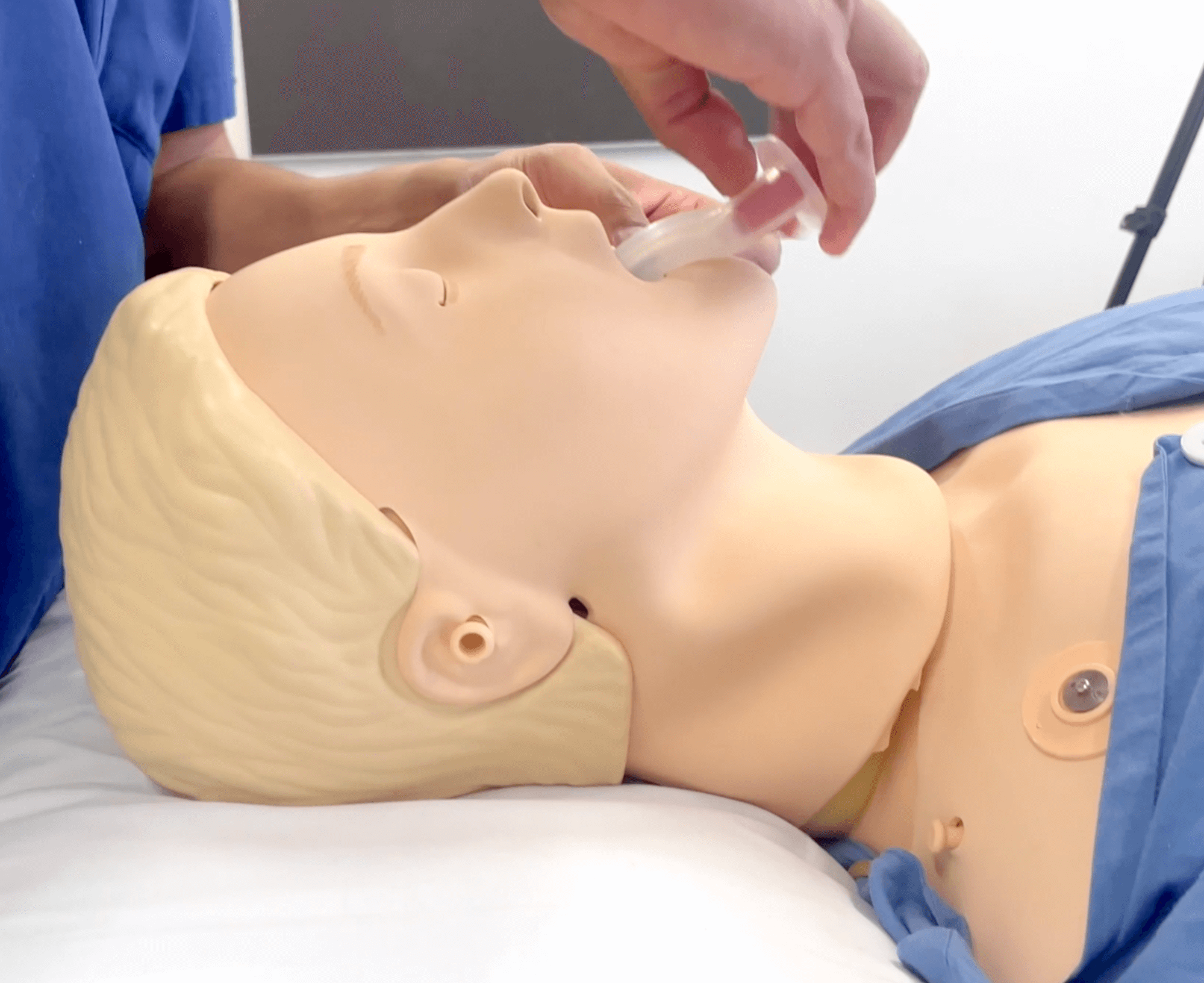
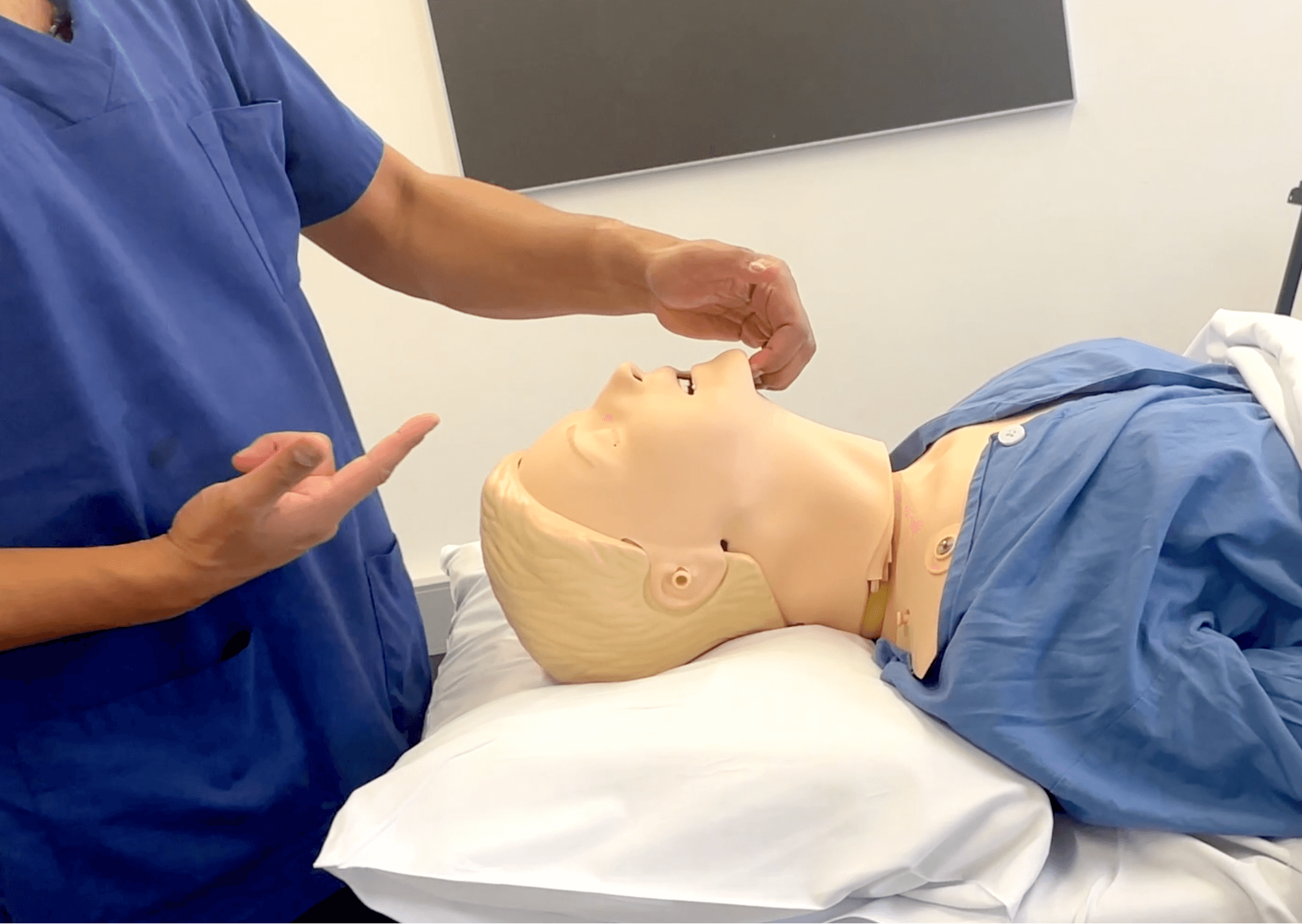
Oropharyngeal (GuedelTM)
- Green, yellow, red (increasing size order)
- Sizing: incisor -> angle of jaw (where it sits inside the mouth)
- Insertion: insert backwards, begin to rotate once halfway in, sweeping the tongue away
- Tip: If it does not fully fit and is properly sized, try jaw thrust whilst gently pushing the rest in.



Guedel’s airway a) insert backwards, once halfway in slowly turn sideways, then insert the rest
Monitoring ventilation
- Look
- Symmetrical rise and fall of the chest
- Paradoxical rise and fall (‘see-saw’ breathing) – indicates obstruction
- Fogging of the mask
- Auscultate
- Measure
- etCO2 (can be attached to the BMV apparatus)
- SpO2 (later sign – due to O2 reserve)
For more information you can view the video on the ABCs of Anaesthesia YouTube page:
[The SUPER DETAILED guide to Bag Mask Ventilation]Test Yourself
Case 1. An obese, bearded male smoker is undergoing laparoscopic cholecystectomy under general anaesthesia. Whilst awake the optimal sats reached are 95%.
Q1) While the patient is awake, what techniques can be used during pre-oxygenation?
Q2) Pre-oxygenation is complete with ETO2 of >80%, sats of 100%, sedation and paralysis is being given. The patient has a poor oxygen reserve and you want to ensure the patient receives good ventilation prior to intubation. What are some techniques to optimise bag mask ventilation?
Q3) As the paralytic agent kicks in, the patient becomes easier to BMV. The anaesthetist attempts to intubate but is unsuccessful on the 1st pass. What are the immediate next steps?
Potential Answers
A1
- Size the mask: fits over the nasal bridge and under the mental prominence
- Positioning: ‘sniffing’ position
- The Grip: double CE grip (gentle pressure)
- Reduce air leaks
- Tegaderm around the mouth to reduce air leak (I’ve personally never had to use this)
- If ongoing air leaks, ask an assistant to apply gentle pressure over air leaks
- If ongoing issues, beard may need to be shaved
A2
- Manoeuvres: jaw thrust + head tilt
- The Grip: double CE grip -> if not working, vice grip
- Assistant to help bag the patient
- If not maintaining sats, airway adjuncts: Guedel (large, bearded male) +/- NPA
A3
- A paralysed patient can NOT breathe for themself
- Go back to basics -> continue optimisation of BMV
- Consider an LMA with optimisation
- Retry ETT insertion using BURP, Bougie, new “Blade”/ video laryngoscopy
Congrats, you successfully ventilated the patient whilst they were intubated using video laryngoscopy. A surgical airway was avoided!